Abdominal Pain: Diverticulitis, stomach ulcer, gastritis, gallbladder pain, and GERD—symptoms and treatments
Abdominal Pain:
Diverticulitis, stomach ulcer, gastritis, gallbladder pain, and GERD—symptoms and treatments

The human digestive system plays a unique role in utilizing nutrients and glucose that feed all the cells of the body. The interplay between the separate organs–each with a unique function–sustains and enhances life. But the digestive system is prone to random and sporadic upsets.
INTRODUCTION: DISORDERS OF THE DIGESTIVE SYSTEM
Through the digestive process, what we eat and drink transforms into the vital nutrients our bodies need to survive and thrive. This feat is accomplished through the mechanical and chemical processes of our digestive system. Each organ of the system—esophagus, stomach, pancreas, gallbladder, liver, and small and large intestine—plays a role.
Ultimately, digestion breaks down and transfers nutrients into the bloodstream for the body’s use, with leftover wastes eliminated through bowel movements.
However, a number of common medical conditions—among them gastroesophageal reflux disease (GERD), stomach ulcers, kidney stones, and irritable bowel syndrome (IBS)—can plague the individual organs, disrupting the entire process. A better understanding of these issues, and their treatments, can help you protect your digestive system and keep it running smoothly.
I. THE ESOPHAGUS
The esophagus is an inch-wide muscular tube, 8 to 10 inches long, that connects the throat and stomach. It is situated behind the trachea (windpipe) and heart. A muscular valve at the top, called the upper esophageal sphincter, prevents food from entering the trachea.
The lower esophageal sphincter is where food passes into the stomach. Ideally, when not eating and drinking, the lower valve remains closed, keeping digestive acid in the stomach.
Common Esophageal Problems
Symptoms will lead you to the esophageal ailment you may be experiencing. Among the common problems are gastroesophagael reflux disease (better known as GERD), Barrett’s Esophagus, dysphagia, and Eosinophilic Esophagitis (EoE).
Gastroesophageal Reflux Disease (GERD) Symptoms: If you have regular bouts of “heartburn”—a sharp, burning feeling in the chest—you may have developed GERD. This is a condition where stomach acid flows back (reflux) up into the esophagus, burning the esophageal lining. If the condition persists, bleeding, scarring, and narrowing of the esophagus can result.

Gastroesophageal reflux disease (GERD) results when a weakened esophageal sphincter at the bottom of the esophagus fails to close properly, allowing stomach acid to back up into the esophagus.
GERD occurs when the lower esophageal sphincter (LES) becomes weak or defective and doesn’t close properly. An overly full stomach, a hiatal hernia, or even pregnancy can cause this. Certain drugs may cause the valve to leak, such as beta-agonists, calcium channel blockers, some antihistamines, and sedatives.
Risk factors for GERD include foods that can weaken the LES. These include chocolate, peppermint, fatty foods, caffeine, and alcohol. Being overweight or obese also puts you at risk for GERD.
Other than persistent heartburn, GERD symptoms include chest pain, trouble swallowing, or difficulty keeping food down. Some people can detect the resulting acidic fluid in their mouths; it has a metallic taste and can cause bad breath. GERD can also cause a sore throat, dry cough, or hoarse voice.
Your doctor will need to perform tests to confirm a GERD diagnosis. Common screening methods include endoscopic exams of the esophagus and stomach or a biopsy of tissue. Your doctor also may perform tests to check the function of the LES or the volume of acid your stomach produces.
To Treat GERD
Eat small, frequent meals over larger, less-frequent ones. Over-the-counter drugs can help; they come in three categories:
- Antacids, which contain components that neutralize acid.
- H2 blockers, which decrease production of stomach acid.
- Proton pump inhibitors (PPIs), which block enzymes necessary for acid secretion.
Stronger drugs are available by prescription.
If these treatments don’t alleviate symptoms, a surgical or endoscopic procedure is a last resort. During the standard procedure, called fundoplication, the upper part of the stomach is wrapped around the lower part of the esophagus (like a hot dog in a bun) to prevent reflux.
Another approach uses an endoscope through which a thin tube is guided to the lower end of the esophagus (just above the stomach). A balloon at the end of the tube is inflated and high-frequency radio waves are delivered to the sphincter muscle. This tightens the muscle, preventing stomach acid from leaking.
During a transoral, incisionless fundoplication, the LES is reconstructed. Because there are no incisions, recovery time is usually shorter than with the traditional procedure.
Certain preventative measures can discourage GERD. Among them: avoiding troublesome food and drink, maintaining a healthy weight, and sleeping with the head of the bed slightly elevated.
Barrett’s Esophagus: A small percentage of people with chronic GERD develop a precancerous condition called Barrett’s esophagus. Long-term exposure to acid damages the esophageal lining, which in some people leads to cancer (called esophageal adenocarcinoma).
Barrett’s esophagus occurs about three to five times more often in people with GERD. Men are about twice as likely as women to be affected, and the typical patient is usually over age 60. Being overweight or obese is also a risk factor for Barrett’s esophagus.
Barrett’s esophagus cannot be diagnosed by symptoms, a physical examination, or blood tests. The only way to diagnose it is with an endoscopy. During the procedure, the physician will take multiple samples of tissue (biopsies) from the esophageal lining. These are examined under a microscope for cellular changes that indicate dysplasia (abnormal tissue) or cancer.
People with Barrett’s esophagus use the same treatment methods for GERD. Since there is no solid evidence that controlling the symptoms of heartburn with medicine or surgery reduces the risk of developing cancer, patients with Barrett’s esophagus must be monitored.
If a biopsy shows high-grade dysplasia (which is more likely than low-grade dysplasia to become cancer), endoscopic ablation therapy either burns or freezes the abnormal cells. An endoscopic mucosal resection removes the lining harboring the cells. A technique called radiofrequency ablation (RFA) uses thermal energy (heat) to destroy the cells. If cancer is found, surgery will be required.
You may be unable to prevent Barrett’s esophagus, but careful monitoring and following the same preventative measures for GERD are solid options.
Dysphagia: The inability to swallow easily or at all, dysphagia can stem from neurological issues or structural problems in the esophagus. Dysphagia can also be a symptom of GERD.
Muscular diseases like Parkinson’s disease, Huntington’s disease, multiple sclerosis, amyotrophic lateral sclerosis (Lou Gehrig’s disease), muscular dystrophy, and myasthenia gravis can cause, or increase risk factors, for dysphagia. All of these conditions weaken or damage the muscles used for swallowing.
Symptoms of Neurologic Dysphagia
They include nasal regurgitation (fluid or food coming out through the nose) and an inability to tolerate both liquids and solids. Symptoms of structural dysphagia begin with intolerance of solids and progresses to intolerance of liquids.
A barium swallow is one screening method for diagnosing dysphagia. This involves drinking liquid containing barium, which coats the lining of the esophagus and highlights any abnormalities in subsequent x rays. An endoscopy, using a small video camera and a light at the tip of the tube, allows the physician to view the inside of the esophagus on a monitor.
Treatments for dysphagia include drugs to relax esophageal muscles, Botox injections, rehabilitative therapy, or surgery to remove nodes or other blockages. Surgery can sometimes ease swallowing by slightly lifting the larynx (voice box). You may need a stent to permanently hold open a blocked or narrowed area.
Most of the underlying causes of dysphagia cannot be prevented.
Eosinophilic Esophagitis (EoE): EoE is an inflammatory condition where white blood cells called eosinophils build up in the lining of the esophagus.
The exact cause of this build-up is not known, but one theory is that it is a form of an allergic reaction, since increased production of eosinophils is associated with allergic conditions, such as asthma, allergic rhinitis, and atopic dermatitis.
Symptoms of EoE include difficulty swallowing (dysphagia), heartburn, and chest pain. An endoscopy can reveal signs of eosinophils and provide a biopsy to confirm the diagnosis.
Treatment for EoE usually includes dietary changes. If the inflammation is caused by a food allergy, an elimination diet may be required or an allergist may perform skin tests to reveal the offending substances.
EoE may also be treated with medications, such as the steroid drug fluticasone, or with PPIs.
II. THE STOMACH
Located slightly on the left side of the body, just below the diaphragm, the stomach is a balloon-type organ that opens at the end of the esophagus and empties into the duodenum, the first section of the small intestine.
The inner lining of the stomach is covered in gastric folds that allow it to expand to accommodate what you ingest. Initially, the stomach stores the material for a while, during which its gastric juices (digestive enzymes, mucus, and hydrochloric acid) begin the digestive process. This delay allows the pancreas, gallbladder, and liver to prepare for their digestive tasks that follow.
Common Stomach Problems
Gastritis: Gastritis is not a single disease, but a condition with several possible causes. The term “gastritis” means inflammation of the stomach lining. When the body’s immune system detects injury (from infection or other causes), it produces inflammation, which triggers processes that promote healing (such as scarring). Healing occurs as the inflammatory process abates. If the cause of injury persists, the immune response continues, causing ongoing detrimental inflammation.
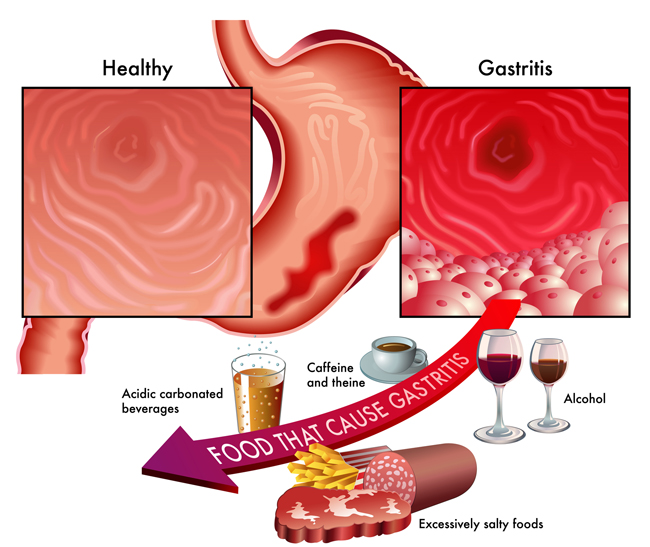
Gastritis means inflammation of the stomach lining but it might actually be caused by several different conditions.
Possible causes of gastritis include too much alcohol, prolonged use of nonsteroidal anti-inflammatory drugs, or infection with the Helicobacter pylori (H. pylori) bacteria. Such diseases as pernicious anemia, autoimmune disorders, and chronic bile reflux can also cause gastritis.
The most common symptoms of gastritis are upset stomach, indigestion, and pain in the upper abdomen that can radiate to the back. Other symptoms are belching, nausea, vomiting, loss of appetite, a feeling of fullness, or burning sensations in the upper abdomen.
Your doctor may suspect gastritis from your symptoms, but an endoscopy and biopsy of the stomach lining may be necessary for an accurate diagnosis.
Treatment for gastritis will depend on the cause. If H. pylori is the culprit, antibiotic drugs will be prescribed. Research suggests that eradicating H. pylori in people with chronic gastritis may reverse the damage to the lining of the stomach that can lead to cancer. For most types of gastritis, drugs to reduce stomach acid are prescribed to promote healing.
Methods to prevent gastritis will depend on the cause. If the source is prolonged use of NSAIDs, these medications should be discontinued. Similarly, if overuse of alcohol is to blame, the solution is to stop drinking.
What Is an Ulcer?: A peptic ulcer is a sore that forms in the lining of the stomach (gastric ulcer) or the first section of the small intestine (duodenal ulcer). Gastric ulcers can occur anywhere in the stomach but are most common in the lower part of the stomach (called the antrum). Duodenal ulcers occur in the first few inches of the small intestine (the duodenum).
Ulcer symptoms
It usually begins with a burning sensation in the upper to middle abdomen within one to two hours after a meal. Other symptoms of an ulcer may include:
- Pain that feels like a dull, gnawing ache
- Pain that is intermittent or constant, lasting for days to weeks at a time before subsiding
- Pain that strikes in the middle of the night, or any other time the stomach is empty
- Pain that decreases after meals
Some symptoms warrant emergency medical attention because they indicate that the ulcer has caused a perforation in the stomach or duodenal wall, broken a blood vessel, or blocked the path of food leaving the stomach and entering the intestine. If you experience any of the following symptoms, seek medical help right away:
- Sharp, sudden, persistent stomach pain
- Bloody or black stools
- Bloody vomit or vomit that looks like coffee grounds
In the past, it was thought that \ stress, spicy foods, or an overabundance of stomach acid caused ulcer symptoms. It’s now known that among the main causes of ulcers is an infection with the bacterium H. pylori. Long-term use of NSAIDs also can cause ulcers. Older adults are more likely to have ulcers, which may be because they have a higher infection rate with H. pylori or because they use more NSAIDs.
To diagnose an ulcer, the first test performed will probably be either an upper gastrointestinal (GI) series or an endoscopy. An upper GI series is an X-ray of the esophagus, stomach, and duodenum. If there is an ulcer, testing for H. pylori bacteria follows.
Ulcer treatment can be highly effective. The three goals to treat ulcers caused by bacteria are to reduce stomach acid, protect the stomach lining, and kill the bacteria. This triple therapy allows the ulcer to heal and lowers the chance that it will come back. Antibiotics are used to destroy the bacteria. Reducing stomach acid is generally accomplished with a proton pump inhibitor (PPIs) and sucralfate and bismuth are typical medications to protect the stomach lining.
III. THE GALLBLADDER
The gallbladder is a small, pear-shaped pouch beneath the liver. The liver produces bile (a combination of water, acid, cholesterol, bilirubin, and lecithin), to digest fats in the small intestine. As the bile is produced, the gallbladder stores it until needed. When you eat fat, the gallbladder sends bile through a system of tubes (called ducts) leading into the small intestine, where it breaks up (emulsifies) the fat.
Symptoms of Gallbladder Problems
Gallstones: If there is too much cholesterol or bilirubin in bile, it can form crystals that clump together into gallstones. A problem arises when a gallstone gets caught in a duct and blocks the normal flow of bile. This causes inflammation of the gallbladder, a condition called cholecystitis.

The gallbladder (green) rests beneath the liver and secretes bile that aids in digestion. The pancreas (yellow) also secretes digestive fluids that aid in the breakdown of food.
Women between ages 20 and 60 are much more likely to develop gallstones than men. After age 60, the disparity between men and women disappears. Excess estrogen appears to increase cholesterol levels, which may explain why women taking birth-control pills or hormone therapy have higher risks.
Diabetes, being overweight, or losing a lot of weight quickly all raise your risk of gallstones. Genetics also play a role: Native and Mexican-Americans have a strong genetic predisposition for gallstones, as does anyone with a family history of gallstones.
If the stone is stuck in the common bile duct, bile can back up and enter the blood, causing jaundice, a condition where the skin and whites of the eyes appear yellow.
To diagnose gallstones, your doctor will probably do an ultrasound or a test called a cholescintigraphy. The patient is injected with a radioactive dye, and a gamma ray camera tracks the flow of the dye into and out of the gallbladder. Additionally, blood tests may be used to look for signs of infection, obstruction, or jaundice.
Symptoms of gallstones
- Severe pain in the upper-right side of the abdomen (called biliary colic) that waxes and wanes and lasts from 30 minutes to several hours
- Pain that radiates to the back, between the shoulder blades, and under the right shoulder
- Nausea or vomiting
- Sweating, fever and chills
- Clay-colored stools
- Dark-colored urine
If the symptoms are severe or suggest acute inflammation (fever), surgery may be required. Gallbladder removal is one of the most commonly performed surgical procedures in the United States. A laparoscopic cholecystectomy requires only small incisions and produces minimal scarring.
If the pain from gallstones is mild and intermittent, simply avoiding fatty foods may prevent or reduce the pain episodes.
IV. THE PANCREAS
The pancreas is located behind the stomach and close to the upper portion of the small intestine. The digestive fluids produced in the pancreas travel from the pancreas to the small intestine via a tube called the pancreatic duct. The pancreas supports the small intestine by producing enzymes needed to help digest fats, proteins, and carbohydrates.
The pancreas also manufactures the hormones glucagon and insulin, hormones that control glucose levels in the bloodstream. If insulin production is impaired, the result is too much glucose in the blood (diabetes).
Common Pancreatic Problems
Pancreatitis: Pancreatitis is an inflammation of the pancreas that can be either short-lived (acute) or long lasting (chronic). While chronic pancreatitis tends to be more serious, either type can cause dangerous complications. Excessive alcohol is known to cause pancreatitis. Or a gallstone from the gallbladder may lodge in the bile duct in such a way that it blocks the pancreatic duct, trapping digestive enzymes inside. The enzymes may begin to digest pancreatic tissue, leading to inflammation.
In addition to gallstones and alcohol, acute pancreatitis can also result from certain types of prescription drugs raise the risk of pancreatitis. Corticosteroids (anti-inflammatory drugs), thiazide diuretics (for high blood pressure) and azathioprine (to prevent kidney rejection post transplant and to treat inflammatory bowel disease) can cause pancreatitis. Smoking increases the risk for both acute and chronic pancreatitis, as does excess abdominal fat.

The pancreas plays a fascinating dual role in human digestion: It secretes enzymes that break down food, and also insulin that allows blood sugar to move efficiently to the cells, where it can fuel the energy needed for survival. The inflammation caused by pancreatitis compromises these important functions.
Symptoms of acute pancreatitis include pain in the upper abdomen that comes on gradually or suddenly and lasts a few days. The pain may radiate to the back. Sometimes pain worsens after eating. Other symptoms are nausea, vomiting, fever, and rapid pulse. Severe cases may impact the heart, lungs, or kidneys. With a chronic condition, symptoms include nausea, vomiting, weight loss, and greasy or oily stools.
Diagnosis of acute pancreatitis requires testing blood for the digestive enzymes amylase and lipase. In patients with acute pancreatitis, extremely high numbers of these enzymes appear in the blood. The doctor may also perform an abdominal ultrasound or a CT scan. These can help detect whether the cause is gallstones, rather than pancreatitis.
Pancreatitis is often treated with fasting for several days to rest the pancreas. Intravenous nourishment may be necessary if pancreatitis persists. Sometimes an extended hospital stay is required. If alcohol is the cause, the patient must completely abstain from alcohol. If gallstones are the source, the gallbladder may need to be removed.
In chronic pancreatitis, the inflammation persists and does not resolve on its own. Some people have a hereditary form of chronic pancreatitis, which can begin in childhood but not be detected until many years later. People with two or more family members who have pancreatitis are at increased risk. The chronic form can so damage the pancreas that the patient may develop diabetes.
Treating acute, painful episodes of chronic pancreatitis is similar to treating acute pancreatitis. Medications will be used to relieve the pain. A nerve block of the main nerve plexus behind the pancreas is useful for relieving pain. Complete abstention from alcohol and a special diet are required to prevent the painful episodes.
V. THE LIVER
The liver is the second-largest organ in the body, behind only our skin. It is located in the upper-right side of the abdomen and it plays an important role in digestion, producing bile to help break down fats and fat-soluble vitamins so the body can utilize them. It has other crucial functions as well, such as removing toxins from the blood, producing immune agents to control infection, and making proteins that regulate blood clotting.
Common Liver Problems
Cirrhosis: When liver tissue becomes inflamed, thickened, and scarred, it cannot preform its essential function. The body cannot survive without the liver processes. Cirrhosis is deadly and kills 25,000 to 30,000 people a year in the U.S.
Alcoholism damages the liver by impeding the metabolism of protein, fats, and carbohydrates. It is the leading cause of cirrhosis followed by hepatitis C in the U.S. and hepatitis B worldwide. Other causes for cirrhosis are rare.
In the early stages there are few symptoms. As it advances, symptoms of fatigue, weakness, weight loss, abdominal pain, and spider-like veins on the skin appear. Eventually, edema (swelling) affects the legs and trunk, and the skin and eyes take on a yellow tone from jaundice.
Although cirrhosis is usually diagnosed from the symptoms, a physical exam that presents a hard, enlarged liver, and laboratory tests that reveal specific enzymes will support the diagnosis. A needle biopsy will confirm the condition beyond doubt and a CT scan, ultrasound, or MRI can help determine the extent of the damage.
Cirrhosis is irreversible so treatment is directed toward stopping the progression and managing symptoms and complications. If alcoholism is the cause, the first step is to completely abstain from alcohol. In fact, no one with cirrhosis, regardless of the cause, should ever drink alcohol. If cirrhosis is caused by hepatitis, this will require medication specific to the type.
People with cirrhosis should eat a diet rich in fruits, vegetables, whole grains, and beans and low in fat, sodium, and animal protein to decrease buildup of toxins. Light exercise is also recommended. Treating symptoms may include diuretics to reduce edema. In severe, uncontrollable cases, a liver transplant may be the only option.
Hepatitis: Hepatitis is an inflammation of the liver generally caused by viral infection. Certain medications, such as acetaminophen (Tylenol), can cause drug-induced hepatitis. An inflamed liver becomes swollen and tender, which can impair or permanently damage the organ.

Hepatitis in all its forms can impact the vital function of the liver.
The hepatitis viruses are identified as A, B, C, D, and E. Any of these viruses can cause short-term (less than six months) inflammation of the liver. Hepatitis A, B, and C may cause no symptoms or just flu-like symptoms (fatigue, nausea, fever, loss of appetite, stomachache, and diarrhea). Some people have dark-yellow urine, light-colored stools, or yellowish eyes and skin. Hepatitis A, B, and C can be detected with a blood test.
Chronic hepatitis B and C take the heaviest toll on Asians, Pacific Islanders, and African-Americans in the U.S. Infection with these viruses account for nearly half of all liver transplants.
Hepatitis A is spread by personal contact or consuming food or water contaminated with human saliva or feces from someone infected with the virus. This is a problem in parts of the world with poor sanitary conditions so travelers in such regions are at risk. Daycare workers and men who have sex with men are also at risk. Hepatitis A can be prevented with a vaccine.
Hepatitis B can be contracted through contact with the blood, semen, or other body fluid of an infected person. People who travel to countries where hepatitis B is common are at risk of infection but there is a vaccine to prevent infection. Hepatitis B infection can resolve on its own without any treatment. However, sometimes the infection is chronic, and leads to serious liver damage, like cirrhosis.
Hepatitis C is transmitted through contact with the blood of an infected person. This generally occurs when drug users share needles. Hepatitis C is not spread by casual contact. People who had blood transfusions before 1992 are at risk because prior to that there was no test to check blood for the virus. The infection may resolve itself within a few months, but about 75 percent of patients become chronic.
An estimated 3.2 million Americans have chronic hepatitis C. In fact, one out of 33 people—“baby boomers,” born between 1945 and 1965—have the disease and many don’t know they have it. This prompted the Centers for Disease Control & Prevention (CDC) to consider routine screening in this population.
There is no vaccine to prevent hepatitis C. However, there are treatments. Weekly injections of peginterferon (Peg-Intron, Pegasys) and the oral drug ribavirin (Copegus, Rebetol) for up to 48 weeks, is the usual treatment. Drug side effects can include fever, chills, headache, muscle and joint aches, rapid heart rate, fatigue, hair loss, skin rash, nausea, irritability, and depression.
Two newer drugs are being used along with peginterferon and ribavirin are boceprevir (Victrelis) and telaprevir (Incivek). They have been shown to boost cure rates and, in some patients, to reduce treatment time.
Obesity raises the risk for failure for this treatment. Weight loss, and treatment for underlying cause, may increase the chances for successful treatment.
Hepatitis D is transmitted through contact with blood from a person infected with the hepatitis D virus. However, it only occurs in people who are already infected with hepatitis B. Hepatitis D can be treated with the drug alpha but there is no vaccine to prevent it.
VI. THE SMALL INTESTINE
The small intestine is approximately 20 feet long and connects the stomach to the large intestine. It does most of the digestive work, breaking down food matter and absorbing the majority of available nutrients.
Small Intestine Problems
Lactose intolerance: During normal digestion, lactose, the predominant sugar in dairy products, is broken down in the small intestine into glucose to be used by the body. An enzyme called lactase, produced in the small intestine, is responsible for breaking down lactose. In lactose intolerance, there is a shortage of the lactase enzyme.

Go easy on the milk if you or your doctor suspect lactose intolerance is causing your stomach pain and bloating.
Lactose intolerance is not dangerous, but it can cause great discomfort. Undigested lactose ferments in the small intestine or colon and can cause such symptoms as nausea, cramps, bloating, gas, and diarrhea. The symptoms usually occur about 30 minutes to two hours after eating or drinking foods containing lactose.
Lactose intolerance may have a distinct cause, such as a disease or injury to the small intestine. However, in most people, it’s genetic and develops slowly over time with no obvious cause. An estimated 40 percent of the world’s population is lactose intolerant; Asian-Americans, African-Americans, and Native Americans are particularly prone.
The condition can be diagnosed with tests that measure the absorption of lactose in the small intestine. The lactose intolerance test involves drinking milk or other lactose beverages then testing the blood glucose level. The hydrogen breath test is another measure as high hydrogen shows lactose is not being digested properly.
Lactose intolerance can’t be cured, but avoiding or limiting milk products manages it. Lactase enzymes are also available to prevent the symptoms for people who react to even small amounts of lactose and wish to continue eating dairy. These are available without a prescription.
Celiac Disease: An essential process in digestion is the absorption of nutrients from the small intestine into the bloodstream. Disorders that interfere with this are called malabsorption disorders, and one of the most common is celiac disease. This condition, also called sprue, is where damage to the small intestine impedes absorption. The damage occurs when the immune systems mistakes the protein gluten for a dangerous intruder and attacks it. This causes inflammation that irritates and damages the small intestine.
The exact cause of celiac disease is not understood, although there is a genetic component; it occurs in five to 15 percent of the offspring and siblings of a person with celiac disease. Occurrence of the disease is on the rise; one in 133 people in the U.S. are affected. A new study indicates that celiac disease has increased in North America from 11.1 percent in 2000-2001 to 17.3 percent in 2008-2010. It can occur at any time in life; in adults it can be triggered by emotional stress.
Symptoms of celiac disease
- Chronic diarrhea
- Anemia (iron deficiency)
- Recurring abdominal bloating, gas, and pain
- Weight loss
- Bone and joint pain
- Muscle cramps
- Pale, foul-smelling stool
- Behavior changes
- Tingling and/or numbness in the legs
- Fatigue
- Mouth sores
- Itchy skin rash (called dermatitis herpetiformis)
- Seizures
If celiac disease is suspected, your physician can make the diagnosis with a blood test and possibly an endoscopic biopsy. The blood test can show whether the body’s immune system is making antibodies against gluten or other enzymes involved in the disease process. Antibodies are substances that are produced by the body to attack threatening invaders. Gene testing to help identify a genetic predisposition to the disease is also available.
Because of the genetic predisposition to celiac disease, relatives, particularly parents, siblings, and children of celiac disease patients also should be tested.
The treatment for celiac disease is to avoid all gluten. Once gluten is removed from the diet, immune reaction to gluten is reduced and the inflammation resolves. The small intestine begins to heal, and absorption of nutrients goes back to normal. For older adults, the small intestine should be completely healed after two years on a gluten-free diet.
Confirmation of celiac disease diagnosis is important since strict adherence to a gluten-free diet can eliminate the symptoms and prevent complications that can occur with this disease. Left untreated, the damage to the small intestine can put people at risk for cancer in the intestine, osteoporosis, anemia, seizures, and liver disease.
Following this diet can be a challenge as it requires avoiding all wheat, rye, barley, and, possibly, oats. This means no pasta, cereal, and bread made with these grains. Instead, celiac patients must find pasta and bread made of potato, rice, soy, or bean flour. Many stores now carry gluten-free products. Check labels carefully to avoid hidden sources of gluten in some products, including additives like modified food starch, preservatives, and stabilizers.
A gluten-free diet requires a substantial change in dietary habits. A dietitian with good knowledge of this disease can provide assistance, particularly following the initial diagnosis. Support groups also can be helpful.
VII. THE LARGE INTESTINE
The large intestine, also known as the colon, is a multi-layered tube approximately 5 feet long that absorbs liquid from the waste material passed down from the small intestine. The bacteria that live in the large intestine take in any remaining nutrients in the stool before it moves into the rectum to be expelled through the anus.
Large Intestine Problems
Constipation: As undigested food passes through the colon, water is absorbed to form the solid waste (stool). If not enough water is removed diarrhea will result. If too much water is removed, the stool becomes hard, dry, and difficult to pass out of the body—constipation.
Many people believe they are constipated if they don’t have a bowel movement every day. In fact, the frequency of bowel movements considered normal ranges from three times a day to three times a week.
Constipation means passing small amounts of hard, dry stool, usually less than three times a week, and straining to have a bowel movement. Other symptoms are bloating, general discomfort, and sluggishness. Like diarrhea, constipation is very common and usually lasts only short time. Even so, constipation accounts for about 2 million doctor visits each year in the United States.
Common laxative treatments
- Bulk or fiber laxatives (Metamucil, Citrucel, Fibercon, and Benefiber) serve to hold water in the intestines and soften stool. Patients using these must drink at least eight glasses of fluid (water, juice, milk, coffee or tea) per day to avoid side effects.
- Osmotic laxatives (Milk of Magnesia and MiraLax,) cause the intestines to secrete water into the colon to make stool soft. These also require adequate fluid intake.
- Stool softeners (Colace and Surfak) provide moisture to the stool.
- Stimulants (Correctol, Dulcolax, and Senokot) cause intestinal muscle contractions to help move the stool more quickly. Long-term use is not recommended.
A low-fiber diet, not drinking enough fluids, and lack of exercise are common causes of constipation. Many medications can cause constipation, including pain medications (opioids), antacids that contain aluminum and calcium, calcium channel blockers (for lowering blood pressure), anti-Parkinson’s drugs, antispasmodics, antidepressants, iron supplements, diuretics, and anticonvulsants.
In most cases, constipation is treated with lifestyle modifications, including increasing activity, daily fluid intake, and the amount of fiber (from beans, fruits, vegetables, or grains) in the diet. Laxatives are usually not necessary for mild cases of constipation. However, if lifestyle changes don’t help, the doctor may recommend laxative or enema use for a short time.
What Is Irritable Bowel Syndrome (IBS)?: About 10 to 15 percent of Americans suffer with irritable bowel syndrome (IBS). Characterized by symptoms such as cramp-like abdominal pain, bloating, diarrhea, and constipation, IBS can be uncomfortable and distressing. However, it does not cause permanent harm to the intestines, nor does it lead to intestinal bleeding or serious disease such as cancer.
What makes IBS worse?
- Large meals
- Wheat, rye, barley, chocolate, milk products, alcohol
- Caffeine
- High levels of fructose
- Carbohydrates in foods like wheat, beer, garlic, onions, artichokes, asparagus
- Sugar alcohols such as sorbitol, fruits, cabbage, beans, lentils, and soy
- Insoluble fiber found in wheat and bran
- Large amounts of fat
- Women with IBS may experience more symptoms during their menstrual periods, suggesting that reproductive hormones can exacerbate IBS.
The colon of an IBS patient is more sensitive and reactive. It can react to stimuli by moving contents too quickly through the colon, causing watery diarrhea. The colon can also react by slowing down the movement of contents, causing constipation.
The cause of IBS is not known. IBS is called a functional disorder rather than a “disease.” Women are more susceptible to IBS than men, and it usually begins around age 20. Emotional stress is often blamed for causing IBS, since no physical damage to the colon is detected. However, while stress may worsen symptoms of IBS, other factors are also at play.
Your doctor will need a complete medical history and a physical examination to make a diagnosis. The doctor may perform stool or blood tests, X-rays, or an endoscopy to rule out other possible causes.
IBS can’t be cured, but it can be treated with dietary changes, stress management, probiotics, and antispasmodic, anti-diarrhea and anti-constipation drugs. There are data to suggest that antidepressant drugs, psychotherapy, cognitive behavioral therapy, and hypnotherapy may reduce symptoms of IBS and improve quality of life. Some IBS patients find it useful to review their diets with a registered dietitian or physician.
Inflammatory Bowel Disease (IBD): Inflammatory bowel disease (IBD) is a collective term for abnormal immune system activity in the intestines that leads to inflammation. The two major diseases are ulcerative colitis and Crohn’s disease.
Ulcerative colitis causes inflammation and ulcers in the inside lining of the large intestine (rectum and colon). It affects just the top layer of the intestinal lining (called the mucosa). Crohn’s disease also causes inflammation, usually in the small intestine, but it can affect all areas of the gastrointestinal tract (mouth to anus). Crohn’s disease affects all four layers of the intestinal wall.
The exact cause of IBD is unknown, but some interaction between hereditary factors, environment, and the immune system is probably at work. It’s theorized that the body’s immune system reacts inappropriately to viruses or bacteria in the intestines. The immune system mistakes these for foreign invaders and launches an attack by sending white blood cells to the intestinal lining. This produces inflammation that becomes chronic, damaging the intestine. This reaction is thought to occur in people genetically predisposed to IBD.
The main symptoms of ulcerative colitis are cramp-like abdominal pain on the lower-left side and bloody diarrhea. Loss of appetite, weight loss, nausea, anemia, and fatigue also are common.
Crohn’s symptoms vary depending upon severity and which part of the intestine is affected, but generally include abdominal pain, diarrhea, and bloating. People with either type of IBD also can have symptoms outside the digestive system, such as joint inflammation (arthritis), eye inflammation, or skin, liver, or kidney problems. These symptoms are probably caused by the abnormal immune system response in these patients.
To diagnose IBD, the doctor will start with a medical history, physical examination, and a series of tests, including blood tests and analysis of a stool sample. If ulcerative colitis is suspected, the next step will be flexible sigmoidoscopy or colonoscopy, which allows the doctor to visualize the interior of the large intestine and take tissue samples for laboratory analysis.
If Crohn’s disease is suspected, the doctor may perform an upper GI series to look at the small intestine, or an endoscopy or capsule endoscopy. The doctor may also do a colonoscopy.
Excellent nutrition is critical for IBD patients (especially those with Crohn’s), who have difficulty absorbing nutrients from food. Dietary supplements may also be needed. Although emotional stress does not cause IBD, it may trigger flare-ups so managing stress in your life may help control it.
Anti-inflammatory drugs known as 5-aminosalicylates are the first line of treatment for mild to moderate IBD (both Crohn’s disease and ulcerative colitis.) They help as maintenance medications to prevent relapses.
Patients with more serious illness or flare-ups may require corticosteroids, like prednisone and hydrocortisone. Because of the serious side effects, corticosteroids are only for short-term use. Drugs that blunt the immune response are the third line of defense and are safer for long-term use. However, they can take up to three months to take effect. These medications include azathioprine (Imuran), 6-mercaptopurine (6-MP), and cyclosporine.
The newest drugs for IBD are biologics, genetically engineered compounds derived from human genes that inhibit aspects of the immune system. They have a more targeted action than corticosteroids, which minimizes side effects. The first biologic used to treat severe Crohn’s was infliximab (Remicade). Another in wide use is adalimumab (Humira). It works for moderate to severe Crohn’s disease that has not responded to other drugs.
Surgical removal of the affected portion of the small intestine or colon may be necessary for advanced disease. About 25 to 40 percent of people with ulcerative colitis will eventually have surgery. The main procedure for ulcerative colitis is a proctocolectomy, where the entire colon and rectum are removed. Many patients are able to have the restorative version, which replaces the colon and rectum with a pouch that allows them to have normal bowel movements. Others will require an ileostomy, in which an opening in the abdomen is created to allow stools to pass out of the body. Ulcerative colitis is cured by this surgery.
Two-thirds to three-quarters of patients with Crohn’s will require surgery at some point and entails removing diseased portions of the small intestine. This surgery is limited because the small intestine is essential for adequate nutrient absorption, so only small amounts can be removed. If Crohn’s disease affects the large intestine, a proctocolectomy can be performed. Surgery does not cure Crohn’s as the inflammation can reappear in a previously unaffected portion of the intestine.
Regular colonoscopies with biopsies are required to monitor the state and progression of IBDs.
Diverticulosis and Diverticulitis: Half of Americans older than age 60 have diverticulosis, a condition where small pouches (about the size of large peas), called diverticula, bulge outward from the colon. Diverticulosis is not a disease in itself, but if the diverticula become inflamed or infected, it becomes diverticulitis and requires treatment. From 10 to 25 percent of people with diverticulosis develop diverticulitis.

Diverticulosis is a condition where pockets form in the lining of the colon. Diverticulitis occurs when those pockets become infected and enflamed.
Although the exact cause is unknown, it’s thought that diverticulosis results from a low-fiber diet. It is more common in industrialized countries, such as the United States, England, and Australia. It is uncommon in Asia and Africa, where people eat diets higher in vegetable fiber.
Fiber softens the stool so it can pass easily through the intestines. If the stool is too hard, constipation will result. Straining to move a hard stool puts pressure on the colon, and which causes weak spots to bulge out, creating diverticula
If diverticula become inflamed or infected, it can cause fever, pain or tenderness in the lower left abdomen, and a change in bowel function or blood in the stool. It is unknown why diverticula become infected, but it may stem from stool or bacteria getting caught in the pouches.
As diverticulitis symptoms can also mimic inflammatory bowel disease or infectious gastroenteritis, the doctor will likely perform a CT scan with contrast, to diagnosis the disease.
Diverticulitis is treated with antibiotics and pain relievers. A short stay in the hospital is sometimes required. In a few cases, diverticula burst and require surgery. Surgery may also be necessary if an infection is persistent or very severe.
The best way to prevent trouble with diverticula is to eat a high-fiber diet, including fresh fruits, vegetables, beans, nuts, corn, and whole-grain foods. Wheat bran is often recommended because it passes through your system quickly, decreasing pressure in the intestines. The Dietary Guidelines for Americans recommends 25 grams of fiber per day for women and 38 grams per day for men, Excess weight and lack of exercise also may increase complications associated with diverticulosis.
VIII. RECTUM and ANUS
The end of the large intestine narrows into the rectum, a muscular tube about three to five inches in length. The rectum joins the large intestine to the anus, the opening through which waste is expelled by bowel movements.
Common Rectal and Anal Problems
Proctitis: Proctitis is an inflammation of the lining of the rectum, which has several possible causes. For example, it can be a side effect of radiation therapy for cancer or medications like antibiotics. People with ulcerative colitis or sexually transmitted diseases can also develop proctitis. Bacterial infection, allergies, and injury to the rectum can also be causes.
The most common symptom of proctitis is an urgent need to have a bowel movement, even though little or no stool is passed. Sometimes mucus is passed in the stool, and the condition can also cause constipation, a feeling of rectal fullness, abdominal pain on the left side, and rectal bleeding.
Proctitis is diagnosed with a proctosigmoidoscopy and biopsy. A proctosigmoidoscopy is similar to sigmoidoscopy; it allows the doctor to see inside the rectum. A sample of tissue (biopsy) may be taken during the procedure to look for the presence of infections.
Treatment will depend on the cause. A bacterial infection (such as from a sexually transmitted disease) will be treated with antibiotics. For symptom relief, the doctor may recommend sitz baths (warm-water baths that cover only the hips and buttocks), topical agents such as Cortifoam, or suppositories or enemas of anti-inflammatory drugs.
Hemorrhoids: The word “hemorrhoid” is a medical term for the tissue cushions surrounding blood vessels in the anal area. What most consider a hemorrhoid when anal tissue prolapses through the sphincter muscle, exposing the delicate lining of the rectum. This can lead to bleeding, itching, and irritation.
Hemorrhoids can either be inside the anus (internal) or under the skin around the anus (external). The chief symptom of internal hemorrhoids is bright-red blood on your toilet tissue or in the toilet bowl. If the hemorrhoid protrudes through the anus, it may become irritated and painful. External hemorrhoids may not produce any symptoms unless a blood clot forms within the tissue. In this case, there may be painful swelling or a hard lump may form around the anus.
Increasing hemorrhoid risk
- Straining to expel stools
- Extended time spent standing or sitting
- Chronic constipation
- Passing hard, dry, small stools
- Diarrhea symptoms
- Laxative abuse
A diagnosis will require an examination of the anus and rectum and the doctor may need to use an anoscope (a lighted tube useful for viewing internal hemorrhoids), a proctoscope (which can be used to examine the entire rectum), or a sigmoidoscope (to view both the rectum and lower colon).
Careful cleansing of the anal area is also important, daily and after each bowel movement, while sitz baths (warm-water baths that cover only the hips and buttocks) may be soothing. Using cold compresses and topical creams on the area can ease pain. Procedures in the doctor’s office include tying off the hemorrhoid so it will fall off on its own or sclerotherapy, an injection that will shrink the hemorrhoid. Only about 10 percent of patients need more invasive surgery.
To prevent hemorrhoids, increase your intake of fiber and fluid and get more exercise. These measures will keep stools soft so they pass more easily, which decreases pressure and straining. Also, empty your bowel as soon as possible after the urge occurs, and avoid straining or sitting on the toilet for a long time.
Anal fissures: An anal fissure is a small tear in the lining of the anal canal, the last portion of the rectum where it connects to the anus. A fissure can cause painful bowel movements and bleeding.
The most likely causes of anal fissures are constipation and decreased blood flow to the area. After childbirth, women may develop a fissure, and people with Crohn’s disease are also susceptible.
Once the tear occurs, each bowel movement can be painful, and there may be a small amount of blood in the toilet bowl or on the toilet tissue. The symptoms are similar to hemorrhoids, except hemorrhoids don’t cause pain with bowel movements.
To diagnose an anal fissure, the doctor will examine the anus and anal canal. A fissure can usually be seen without the aid of a viewing instrument. However, in some cases, an instrument called an anoscope may be used.
Treatment usually involves resolving the constipation that caused the tear and promoting healing of the area with gentle cleansing and warm, sitz baths. Anesthetic ointments and topical muscle relaxants also may be used.
IX. DIGESTIVE WELLNESS LIFESTYLE CHOICES
Diet: You cannot expect good performance from your digestive system if you don’t supply it with high-quality, compatible fuel. If you have yet to do so, adopt these healthy eating habits.
- Eat at least seven daily servings of fruits and vegetables to help fight off disease.
- Whole grains are your best choice. If “whole grain” isn’t the first or second item on the ingredient list, pass it by.
- Choose fish or poultry over red and processed meats. Animal fat puts undue strain on your digestive tract.
- Instead of frying, try steaming, poaching or microwaving your foods to preserve nutrients and avoid carcinogens that form in high heat.
- Go easy! Instead of eating three large meals a day, eat six small meals instead.
Fiber has been mentioned a few times in this report. It is a known fact that increasing fiber in your diet can prevent, or alleviate, certain digest tract issues, such as:
- Chronic constipation or constipation pain
- Diverticulosis
- Hemorrhoids
- Irritable bowel syndrome symptoms (depending on whether constipation or diarrhea is present
A high-fiber diet also can help lower cholesterol, prevent obesity, heart disease, and colorectal cancer.
There are two types of fiber: insoluble and soluble. Insoluble fiber includes wheat bran, whole grains and whole-grain products, including breads and cereals, and some vegetables. Soluble fiber is found in beans, fruit, oats/oat bran, nuts, seeds, and vegetables.
While the average American takes eats only 15 grams per day, the recommended dietary fiber intake is 25 grams for women and 38 grams for men.
If you are concerned about excess gas, increase your fiber intake slowly. Also, as you up your fiber intake, make sure to drink plenty of liquids.
Be Active: Everyone knows that adequate exercise is necessary to overall good health. This includes a healthy digestive system. At the very least, improved blood circulation from exercise helps every cell receive the oxygen and nutrients it needs to function properly and resist disease.
After getting your doctor’s approval for an exercise program, get at least 30 minutes of moderate to vigorous exercise most days of the week.

If you want to keep moving, you need to get moving
Manage Stress: As mentioned throughout this report, excess emotional stress affects digestive health. Pinpoint your personal stress triggers and do what is necessary to alleviate, or at least minimize, them.
If you have trouble accomplishing this on your own, seek guidance from your doctor or a professional counselor. Find ways to work calming routines into your daily activities, such as taking a walk in nature or just sitting still and being quiet for five minutes at several points throughout the day. Seek out people whose company you enjoy and indulge your sense of humor.
Maintain a Healthy Weight: Being overweight puts undue strain on your entire body, and this report highlighted several digestive conditions that are exacerbated by obesity or excess weight. Adopting a healthy eating plan, cutting down (or cutting out) alcohol, quitting smoking, and getting regular exercise will free your body from many impediments to overall good health.
Preventative Screening: Just as with other regular checkups, the digestive system, primarily the colon, should have preventative exams. The American Cancer Society suggests the following screening guidelines beginning at age 50:
- A flexible sigmoidoscopy every five years or
- Colonoscopy every 10 years or
- Double-contrast barium enema every five years or
- CT colonography (virtual colonoscopy) every five years.
A sigmoidoscopy is an examination of the rectum and colon with a sigmoidoscope, a thin tube with a tiny camera on the end. This allows the doctor to detect any polpys or abnormalities. This procedure can be done in a doctor’s office and does not required anesthesia.
A colonoscopy is a similar procedure, but allows the doctor to visual the entire colon. This procedure is more extensive and the patient usually is placed under light anesthesia.
A double-contrast barium enema uses X rays and an enema treated with barium is inserted into the colon to reveal any abnormalities. The patient is awake and will have to change positions several times for multiple x-rays. The procedure has been around for decades, and is gradually being replaced by CT colonography.
A CT colonography, or virtual colonoscopy, uses low-dose radiation and computed tomography to take pictures of the colon without using invasive techniques.
 SOCIAL ANXIETY
SOCIAL ANXIETY  WHITE COAT SYNDROME
WHITE COAT SYNDROME  Keep Walking to Lower Your Depression Risk
Keep Walking to Lower Your Depression Risk