Medical problems of the eyes, ears, nose, and throat: Glaucoma symptoms, sinus infection, ringing in the ears, vertigo, and more
Medical Problems of the Eyes, Ears, Nose, and Throat:
Glaucoma symptoms, sinus infection, ringing in the ears, vertigo, and more

Our eyes, ears, nose, and throat are our window on the world. Keeping them in optimal condition keeps us connected.
Table Of Contents:
Introduction
I. The Eyes
II. The Ears
III. The Nose
IV. The Throat
Introduction
The eyes, ears, nose, and throat work together and independently to help us perceive our world through sight, sound, scent and taste. These organs play such critical roles in quality of life it is vital to keep them as healthy as possible. A better understanding of the common health issues related to the eyes, ears, nose, and throat, can help you keep them operating at peak performance.
I. THE EYES
Overview
Most common eye diseases—macular degeneration, glaucoma, and cataracts—are age-related. The information in this report can guide you through vision changes as you age. It addresses the most common eye conditions, explaining what to look for and what to do if you develop a vision problem and provides prevention tips to help you avoid loss of vision.
The bony orbit that encloses the eye provides protection and supports the fat and muscles that coordinate eye movements. The white of the eye, the sclera, is a protective collagen coating with an opening in front for the cornea and one in the back for the optic nerve to connect to the brain.
The cornea is the clear, outermost layer that covers the pupil and iris and the anterior chamber, between the iris and the cornea, contains the clear, watery aqueous humor, which conveys nutrients and removes waste, then drains away. The pupil is the opening in the center of the iris, the colorful portion of the eye. The iris is made of muscles that constantly adjust the pupil opening to control the amount of light entering the eye. It opens wider in darkness and narrows in bright light. The lens, just behind the iris and pupil, controls focus, adjusting for near and distant images. Tiny ciliary muscles in the lens contract for near vision and relax for distance, maintaining a focal point on the retina at the back of the eye wall.
The retina is a layered sheet of light-sensitive cells called rods and cones. The central, macula region of the retina is the source of the sharpest images. Chemicals within each cell make them respond to different wavelengths of light, providing colors and contrast. The rods and cones connect to other nerve cells that connect to the brain through the optic nerve. Once light signals reach the visual cortex in the brain, they convert into the images we “see.”
Common Problems
Just as with our other physical abilities, that passing years take a toll on our vision. Particularly, our abilities to discern contrast and to see clearly up close suffer. Yet, these are small issues compared to the eye diseases that can accompany aging. Cataracts, glaucoma, and macular degeneration can cause blindness that leads to loss of independence. Prompt diagnosis and treatment for these issues is imperative.
Age-Related Macular Degeneration
This condition affects the central portion of the retina, the source of the sharpest images. It causes slow erosion of central vision necessary for reading and recognizing faces. Age-related macular degeneration (AMD) accounts for more than half of blindness, and the leading cause of vision loss in Americans over age 65. As yet there is no cure for AMD, so seniors must be vigilant about regular eye exams.
Forms
The first and most common form is dry, or non-exudative. This occurs when degenerated cells from the macula build up under the retina. The only early symptom may be slightly blurred. Dry macular degeneration can progress to the more dangerous wet form.
The less frequent but far more serious wet, exudative form, accounts for most macular degeneration blindness. In wet AMD, abnormal blood vessels grow under the retina, leaking blood and fluid, lifting and damaging the retina. Fortunately, only about 10 percent of age-related macular degeneration progresses to this form. Untreated, wet AMD progresses much faster than dry and requires immediate treatment to preserve vision.
Causes
For unknown reasons, retinal structures break down which some experts believe leads to both dry and wet macular degeneration. Some researchers point to free radicals as the source. Other possible causes are:
- general, low-grade inflammation throughout the body
- genetic markers that increase risks
- high blood levels of a protein called cystatin C
Risk Factors
Smoking, high blood pressure and high LDL cholesterol all raise the risk of developing age-related AMD. Other risk factors that you can control are:
- Dietary factors/poor nutrition
- Obesity
- Heart disease
- Overexposure to ultraviolet light
Risk factors you cannot modify:
- Caucasian race
- Family history
- Female gender
- Light-colored iris
Symptoms
Stage 1 of dry AMD has virtually no symptoms. At this stage, it will likely only be discovered through a dilated eye exam where your doctor may note a few small- or medium-sized drusen (yellow, fatty proteins) under yours retina.
In the second, intermediate stage, there are many medium-sized drusen or at least one large druse, and patients may notice vision problems such as a blurred spot in the center of their vision, or the need for additional light to read.
At stage three, symptoms may become severe. The blurriness in the center of vision grows larger and darker until reading and seeing faces becomes difficult. At this stage, the retina begins to atrophy.
Fortunately, macular degeneration can take many years to compromise vision, and sometimes never progress to Stage 3 at all.
Following are signs of dry macular degeneration:
- Increasing need for bright light when reading or doing detailed work
- Blurry vision
- Mildly distorted vision
- Colors appear dull
With wet macular degeneration, symptoms may appear suddenly and worsen quickly. It is important to get to an ophthalmologist right away if you have any of these symptoms, some of which are also common to dry AMD:
- Distortions in your central field of vision
- Straight lines that appear wavy or objects that look distorted, an important early sign of wet AMD
- Blurred vision
- Colors appear dull
- A central blurry spot or blind spot that may be growing
- Difficulty reading
- Trouble recognizing faces
Once you have macular degeneration in one eye, you face a higher risk of it developing in the other. You will need regular check-ups to monitor the disease progression.
Screening to Diagnose
The Amsler grid looks like a sheet of graph paper. If you look at it and see wavy, broken or distorted lines on the graph, your doctor will note their location and the degree of distortion to determine the location and extent of macular damage. If you have dry AMD, this can help catch the conversion to wet AMD early, when it is more treatable. If you have wet AMD, regular use of the grid can signal the time for your next treatment.
You can use an Amsler grid at home. Cover one eye and look at the grid, then switch and cover the other eye. If you detect any changes in the grid’s appearance, call your ophthalmologist immediately for a dilated eye exam.
A fluorescein angiogram involves injecting fluorescent dye into your blood stream. A photograph of your retina as the dye passes through can detect any leaking blood vessels.
In optical coherence tomography (OCT) a scanner takes cross-sectional images of your retina based on the reflection of light and/or ultrasound waves.
Treatments/Surgery
For dry AMD, it cannot be reverse once it reaches the advanced stage. Fortunately, early dry AMD is usually slow to progress, and most people live normal lives with few vision problems for many years. If you progress to intermediate stage AMD, AREDS supplements (see below) can reduce the risk of further progression. You must monitor your condition using an Amsler grid, and have regular eye exams to check for progression or development of wet AMD.
For wet AMD, drugs called anti-angiogenesis compounds have dramatically improved vision in patients. The most common is Lucentis. Another drug, Avastin, is not FDA approved for AMD treatments, but is often prescribed “off label”. Both are administered by injection into the eye. Lucentis is much more expensive than Avastin, costing as much as $2,000 a dose.
Another option for wet AMD is photodynamic therapy. A relatively painless outpatient procedure, it uses a combination of a non-thermal laser and a light-sensitizing drug to target the abnormal blood vessels. This treatment was safe in long-term studies.
Laser photocoagulation is another treatment for wet AMD that was once the only option available. Only about 15 percent of patients are good candidates for this procedure as it works best on newly formed blood vessels that are not growing into the center of the macula. It takes only about 30 minutes in an ophthalmologist’s office. Unfortunately, some healthy retinal tissue is destroyed in the process.
The original Age-Related Eye Disease Study (AREDS1) by the National Eye Institute established that taking high-dose supplements of vitamins C and E, beta-carotene, copper, and zinc helped slow disease progression. Subsequent research (AREDS2) showed that benefits of the AREDS formula persisted for the decade following the end of the first trial.
Vitamin D also might reduce AMD risk, possibly by reducing inflammation and/or preventing the growth of new blood vessels in the retina. Postmenopausal women with high levels of vitamin D in their blood are much less likely to develop AMD than women with low vitamin D, according to a recent study. There is also evidence that B complex supplements (B6, B12, and folic acid) might help prevent AMD. Women who take these supplements daily may reduce their risk by more than 30 percent.
Prevention
There is no proven way to prevent age-related macular degeneration, but because some risk factors relate to lifestyle, you can reduce your risk. Quit smoking, maintain a healthy weight, and control your blood pressure. Lifestyle factors are so important that women who introduce a few simple changes could cut their risk of AMD by more than two-thirds.
Early treatment may prevent AMD onset, or greatly slow its progress. This is why it is critical to have regular eye exams, especially if you have a family history of AMD, you smoke, and/or you’re overweight. Age-related macular degeneration typically appears after the age of 50. As you age, the odds rise.
AGING EYES
Aging can affect the shape of the eye and/or the functionality of its components. Refractive errors occur when the anatomy, or shape, of the eye prevents light from properly focusing on the retina. Age also affects the eyes ability to produce tears.

As we age it gets harder and harder to see–making early intervention to preserve eyesight a priority.
Forms
The most common forms of refractive errors are nearsightedness, farsightedness, and astigmatism. The most common age-related vision problem is presbyopia, where the eye begins to lose its ability to focus due to loss of lens flexibility. It’s a gradual process that happens to everyone who lives long enough, which usually requires corrective lenses beginning at some point in your 40s. Chronic dry eye is another common condition of aging eyes.
Causes
- Nearsightedness (myopia) occurs when the eye is too long from front to back, causing distant images to fall short of the retina. A nearsighted person has trouble focusing on distant objects but can see close-up objects clearly.
- Farsightedness (hyperopia) -a farsighted person can clearly see distant objects, but close objects are fuzzy. Shorter-than-average eyes cause hyperopia, or farsightedness, where the focal point of close objects falls behind the retina.
- Astigmatism occurs when the cornea is oblong rather than round. This inhibits focus for both near and far objects, leading to distorted vision.
- Presbyopia is the loss of lens flexibility, and thus clear vision, brought on by aging.
- Dry eye syndrome occurs when the eyes don’t produce enough tears, or tears lack the consistency to lubricate the eye. Hormonal changes can trigger dry eye syndrome.
Risk Factors
Although there are no specific risk factors for refractive errors brought on by aging, there are a few for chronic dry eye syndrome. Menopausal women are at greatest risk as hormonal changes affect tear production and increases eye inflammation.
Declining male hormone levels increase risk for men due to deterioration of the tear film, which provides moisture to the cornea. Overuse of the eyes (using a computer or driving a lot), smoking, LASIK surgery, and long-term use of contact lenses are also risk factors for chronic dry eye syndrome.
Symptoms
The first signs of presbyopia, or any refractive errors, may be difficulty reading at your normal distance, and finding yourself holding material farther away to focus, or headaches or eyestrain when reading or doing close work.
Symptoms of dry eye syndrome include aching, redness, stinging, burning, itchiness, and the sense that there’s something in your eye.
Screenings to Diagnose
Many people have their eyes examined by optometrists at discount outlets. This type of exam is fine to determine your eyeglass prescription or pick up new contact lenses. However, it is not thorough enough to diagnose age-related eye diseases, because your eyes are not dilated with drops. Dilating the eyes expands the pupil, and it’s a crucial step in checking for the early signs of eye disease because it gives the doctor a much better view of what’s going on inside your eye.
Treatment
Glasses or contact lenses compensate for distortions by bending light before it enters the eye, so the image focuses correctly and sharply on the retina. The focusing ability of the lens decreases with age, which is why eyeglass prescriptions grow stronger as we get older.
- Bifocals: These glasses correct both distance and reading vision. Typically, a horizontal line across the middle divides the lens into correction for distance, through the upper lens, and for close-up vision, through the lower portion. Progressive bifocals accomplish this without a line.
- Trifocals: These lenses correct for distance, middle-distance (such as looking at your computer screen), and close-up vision.
- Monovision correction: This type of correction uses a contact lens for distance vision in one eye and a lens for close-up work in the other.
- Laser surgery to implant a multifocal lens: This lens can function like a younger eye, adjusting between near and far objects to provide clear vision at all distances. During surgery, the natural lens of the eye is removed and then replaced with the artificial lens.
- LASIK or PRK surgery: Laser-assisted in situ keratomileusis (LASIK) or photorefractive keratectomy (PRK), reshape the cornea to improve near vision.
Most cases of dry eye syndrome are easily treated with over-the-counter artificial tears. You may need to try different formulations to see which one works best. Eye drops containing omega-3 fatty acids might help reduce inflammation.
Severe dry eye may be treated with tiny plugs inserted into the eye’s drainage system. The plugs force tears to back up into the eye, helping maintain moisture.
Prevention
You cannot prevent your eyes from aging, but you can give them the best possible care. The American Academy of Ophthalmology recommends a baseline eye exam at age 40. Your ophthalmologist will exam schedule after that, based on your risk factors.
CATARACTS
The eye’s clear lens consists of protein and water, arranged in a precise pattern. As you age, the proteins clump together, causing the lens to cloud and turn yellow. This is a normal process that occurs in almost everyone. In about half the population, the lens eventually gets too cloudy for clear vision.
Forms
There are three types of cataracts:
- Nuclear cataracts form in the center of the lens and are the most common age-related cataracts.
- Cortical cataracts occur at the edge of the lens and progress toward the center.
- Posterior subcapsular cataracts form at the back of the lens and are more common with injury, long-term steroid use, or diabetes.
Causes
The exact cause for cataracts is unknown, but one likely contributing factor is a class of compounds called oxygen-free radicals. They are generated by natural biochemical processes, notably metabolism, as well as by as well as environmental pollutants, including cigarette smoke. In younger people, these free radicals are sopped up by endogenous antioxidants, but the body’s ability to produce antioxidants decreases with age.
Ultraviolet light also contributes to cataract formation, probably partly by generating free radicals.
Risk Factors
Everyone is at risk for cataracts as they age, but some have greater risks. Women are at high risk than men, especially those who receive hormone replacement therapy (HRT) after menopause.
Smoking also increases the cataract risk, and it can take 10 to 20 years after smoking cessation for your risk to drop.
Taking certain medications, like steroids and some SSRI antidepressants, also may make you more prone to cataracts.
Other risk factors for cataracts include:
- Diabetes
- A family history of cataracts
- A history of eye injury
- Previous eye surgery
- High exposure to sunlight
- High exposure to radiation
Symptoms
The most common symptoms of a cataract are cloudy or blurry vision—as if you were looking through a dirty windshield. Other symptoms include:
- Colors that seem faded or dull
- Increased glare from lamps, sunlight, and headlights, or circles or halos forming around lights at night
- Reduced night vision
- Double vision that does not disappear when the other eye is closed
- Need for more light for reading or detailed work
Screenings to Diagnose
If you have any of these symptoms, you should see an ophthalmologist as soon as possible. The doctor will do a dilated eye exam, complete with a slit lamp examination of the lens, to determine whether you have a cataract and how extensive it is.
Treatments/Surgery
Cataract surgery improves vision more than 90 percent of the time. The surgeon removes the clouded lens and replaces it with a clear artificial lens. If you have cataracts in both eyes, you will need two surgeries several months apart. Cataract surgery is never performed on both eyes on the same day.
Standard cataract surgery, with a technique called phacoemulsification, uses ultrasound to emulsify the cataract so that it can be removed through a tiny incision. An artificial lens replaces the damaged lens.
Femtosecond laser cataract surgery reduces the amount of ultrasound energy needed by nearly half, which eliminates any loss of healthy cells, and uses smaller incisions.
When a lens containing a cataract has grown too dense or hard to treat with ultrasound waves, the doctor will perform a extracapsular cataract extraction. This uses an incision about 3/8 of an inch wide in the cornea, through which the cataract is extracted. The doctor then suctions out the rest of the lens, implants the artificial lens, and closes the incision. The larger incision prolongs healing by several weeks.
Prevention
Cataracts are a natural consequence of aging, however, you can reduce your risk. When out in the sun, wear sunglasses that block 99-100 percent of UVA and UVB rays and/or a hat with a brim to limit your exposure to the sun’s ultraviolet light. Additionally, new research finds that physical activity reduces the risk of developing cataracts. Other preventive steps are:
- Stop smoking
- Reduce your alcohol consumption if you drink heavily
- If you have diabetes, follow your doctor’s instructions and keep tight control of your blood sugar levels
- Eat a healthy diet with at least two-and-a-half cups of fruit and two cups of vegetables a day
There is some evidence that statins, the cholesterol-lowering drugs, might help prevent cataracts. More than one study has found that people who take statins have a significantly lower risk of developing cataracts. Talk with your doctor about this option.
GLAUCOMA
Glaucoma is an eye disease where excess pressure irreparably damages the eye, causing blindness. It is the leading cause of irreversible blindness in the world. In the U.S., an estimated two million people have glaucoma. An equal number of people probably have the disease but don’t know it.
Because symptoms don’t manifest until the disease is very advanced, glaucoma is a sneaky vision thief. Yet, fewer than 10 percent of Americans surveyed know that glaucoma has no warning signs, according to the National Eye Institute.
Glaucoma treatments have improved with fewer side effects. Because doctors can usually control glaucoma once detected it’s important to seek treatment right away and be vigilant about taking your medications.
Forms
The most common form is primary open-angle glaucoma. A malfunction in the meshwork that drains the aqueous humor from the “open angle,” where the iris and cornea meet, is the likely cause. In open-angle glaucoma, the drainage slows, leading to a surplus that builds pressure in the eye, damaging the optic nerve and retina.
Angle-closure glaucoma stems from a congenital malformation of the eye’s drainage system. When this develops, the angle into which the aqueous fluid normally drains becomes blocked. The eye pressure increases so rapidly that vision loss can progress to blindness within just one or two days if not treated aggressively.
Causes
Glaucoma is caused by a build-up of pressure in the eye from excess or blocked aqueous humor. The pressure builds, eventually damages the retina and optic nerve, causing blindness. Glaucoma can also stem from an eye injury, inflammation, infection, a very mature cataract, diabetes, lupus, or certain medications (particularly steroids).
Risk Factors
Everyone over the age of 60 is at increased risk for glaucoma, but the following factors increase risk even further:
- African-Americans over age 40
- Family history of glaucoma
- History of previous eye injury
- History of steroid use
- Diabetes
- Other related health problems, including high blood pressure and migraine headaches
- Thyroid problems
- High cholesterol
Lupus and diabetes are also risk factors for glaucoma. Heart disease is linked to glaucoma. Though high eye pressure is a risk factor and often an early warning sign of glaucoma, it doesn’t necessarily mean that nerve damage is occurring. Some people with high eye pressure never develop glaucoma.
Glaucoma Symptoms
Symptoms for angle-closure glaucoma include:
- Sudden blurry vision
- Severe eye pain or headache
- Nausea and vomiting
- Light sensitivity
- Colored halos forming around lights
If you have any of these symptoms, seek medical attention immediately. Doctors can save your sight with prompt treatment, usually by creating a tiny hole in your iris to relieve pressure. Do not procrastinate, because the damage happens fast, and once vision is lost, it cannot be restored.
Screening to Diagnose
While the “air puff” test can screen for glaucoma by detecting elevated eye pressure, the only way to diagnose it early with certainty is with a full dilated-eye exam, during which the doctor can examine the optic nerve.
A comprehensive glaucoma screening may include one or more of the following tests:
- Tonometry: A more accurate test of internal eye pressure than the eye puff test.
- Slit lamp and hand-held ophthalmoscope: To examine the optic nerve for deterioration.
- Gonioscopy: A special contact lens containing mirrors is used to visualize the angle causing the problem and the extent of blockage.
- Photography: Computerized imaging of the optic nerve to assess damage.
- Visual field testing: Checking your peripheral vision with flashing lights to see how badly your sight has been compromised.
- Pachymetry: Measures the thickness of the cornea to assess your risk of developing glaucoma.
- Heidelberg Retinal Tomography and Optical Coherence Tomography: These create computerized images of the optic nerve that enable clinicians to look for damage.
Treatments/Surgery
Although there is no cure for glaucoma, treatments to lower eye pressure can help control, or delay, vision loss, and blindness. Keeping intraocular pressure at a steady, low level might further reduce the risk of vision loss.
In the U.S., medications are typically the first line of treatment for glaucoma, and a variety of classes and formulations have been developed, most taken as eye drops.
Here are some medication options:
- Prostaglandins improve the drainage of fluid from the eye, and they have the advantage of once-daily dosing.
- Prostamides increase the flow of fluid from the eye. Side effects include red or itchy eyes.
- Beta-blockers reduce the amount of aqueous humor the eye produces. Possible side effects are rare but include difficulty breathing, slowed heart rate and blood pressure, impotence, fatigue, and depression.
- Alpha-agonists, such as Alphagan-P, and iopidine, reduce the amount of fluid produced and increase drainage from the eye. Side effects include irritation, dry mouth, and fatigue.
- Topical carbonic anhydrase inhibitors, including Trusopt and Azopt, reduce the amount of fluid in the eye. In some cases, these drugs can cause burning and blurred vision.
- Miotics work by constricting the pupil and opening the eye’s drainage system, allowing more fluid to pass from the eye. Side effects are blurred vision, headache, extreme nearsightedness, and problems with night vision.
One successful treatment is the use of tiny drains the size of an eyelash, called stents. During a clinical trial, these devices reduced intraocular pressure so stably that after six months, most patients no longer needed eye drops.
Laser surgery may be more effective than medication for controlling intraocular pressure in glaucoma patients with advanced disease who are already taking the maximum doses of medication.
Trabeculoplasty is a type of laser surgery that is performed in 10-20 minutes as an outpatient procedure in a doctor’s office. The doctor uses a high-energy laser to burn holes in the drainage canals to facilitate drainage. You will receive medications to control inflammation, and regular glaucoma drugs.
In selective laser trabeculoplasty the laser targets only selected cells in the eye. It conserves healthy tissues better than conventional laser surgery, while still easing drainage of fluid. Selective laser trabeculoplasty can be performed on an outpatient basis.
Laser surgery is not a permanent solution. In fact, more than half of patients later require conventional surgery because their eye pressure rises within two years after a laser procedure. Because the laser procedure carries less risk than conventional surgery, however, many doctors advise trying it first.
Trabeculectomy is the removal of the eye’s drainage meshwork in an effort to reduce intraocular pressure.
Surgery may allow you to reduce your dosage or delay taking certain medications. But surgery may not eliminate the need for drugs. In more than half of all patients, intraocular pressure rises after surgery, and eventually requires increasing drug doses.
Conventional surgery is usually offered to patients when medications and laser surgery have failed, or if there is significant damage to an untreated eye, or if there is scarring. It works by creating a new alternative drainage system to replace the natural meshwork drain.
For most patients, conventional surgery is effective and long lasting, but it does not always work the first time. About 40 percent of people require a second surgery.
Prevention
Unfortunately, no preventive measures are 100 percent effective. The best option is dilated eye exams and eye pressure checks every one to three years between ages 55 and 64, and every one or two years after age 65.
Recent research shows that people with a long history of moderate exercise may have a reduced risk of glaucoma, suggesting that strength-training exercise can help reduce eye pressure.
Statin drugs, which lower cholesterol, also may decrease the risk of glaucoma. But there is not yet enough evidence to justify taking statins for glaucoma prevention, particularly because these drugs carry their own risk of side effects.
DIABETIC RETINOPATHY
Diabetic retinopathy, a complication of diabetes, afflicts approximately 4.2 million Americans—roughly one-third of whom have diabetes. It is the leading cause of new blindness in people between the ages of 20 and 74.
Forms
Nonproliferative diabetic retinopathy is the disease’s early stage. It begins with tiny bulges in weakened blood vessels of the retina that leak blood and fluid into the retina. More blocked blood vessels characterize moderate nonproliferative retinopathy and during the final, severe stage parts of the retina lose their blood supply.
New blood vessels begin to grow on the retina to bolster the blood supply. This is the most severe stage, called proliferative diabetic retinopathy. Up to 75 percent of people with nonproliferative will progress to the proliferative form within one year
Causes
Diabetes damages tissue throughout your body, including blood vessels in the eyes. Without proper blood flow, the retina and optic nerve incur permanent damage.
The longer you have diabetes, the more likely you will develop retinopathy. The risk rises from 10 percent within five years post-diagnosis to 70 percent after 15 years.
Risk Factors
Everyone with diabetes is at risk for diabetic retinopathy. Your risk increases the longer you have diabetes and the less you control your blood sugar. Other risk factors include:
- High blood pressure
- Obesity
- High cholesterol levels
- Kidney problems
- Infections
Symptoms
Diabetic retinopathy can progress to an advanced stage without any symptoms or pain. If you have any of the following symptoms see your ophthalmologist immediately:
- Dark streaks or a red haze that blocks vision
- Any sense of vision loss or blurred vision
- A blind spot in the center of your vision
- Difficulty adjusting to changes in light
- Spots or “cobwebs” floating in your vision
Screening to Diagnose
Screening methods to check for the extent and location of damaged blood vessels include fluorescein angiogram, where dye injected into the bloodstream highlights damaged blood cells. Another method is optical coherence tomography (OCT) that uses light waves to create clear images of the retina.
Treatments/Surgery
The most common treatment is laser surgery called photocoagulation to stop the leakage and growth of new blood vessels. Photocoagulation can reduce vision loss up to 50 percent.
If bleeding into the vitreous body has blocked your vision, you may need vitrectomy surgery to remove it. This surgery replaces blood-clouded vitreous with saline solution to preserve the shape and pressure of the eye.
The same medications used to treat age-related macular degeneration, Lucentis and Avastin, are used to treat diabetic retinopathy.
Prevention
If you have diabetes, get a dilated eye exam every year. Diabetic retinopathy can be treated successfully if caught early. You can also reduce your risk with these methods:
- Do not smoke. Smoking shuts down blood vessels
- Lower your cholesterol and lipid levels
- Control your blood sugar
- Be alert for any vision changes
II. THE EARS
Overview
To appreciate vast combinations of musical notes, the varied complexities of communication, and the multitude of other rich sounds of our world, requires a delicate, intricate instrument: the human ear.
The delicate structures of the middle and inner ear are prone to problems as we grow older–from degradation of the hearing bones to the fluids inside the cochlea. Your ears and surrounding structures are responsible for hearing but also balance and stability.
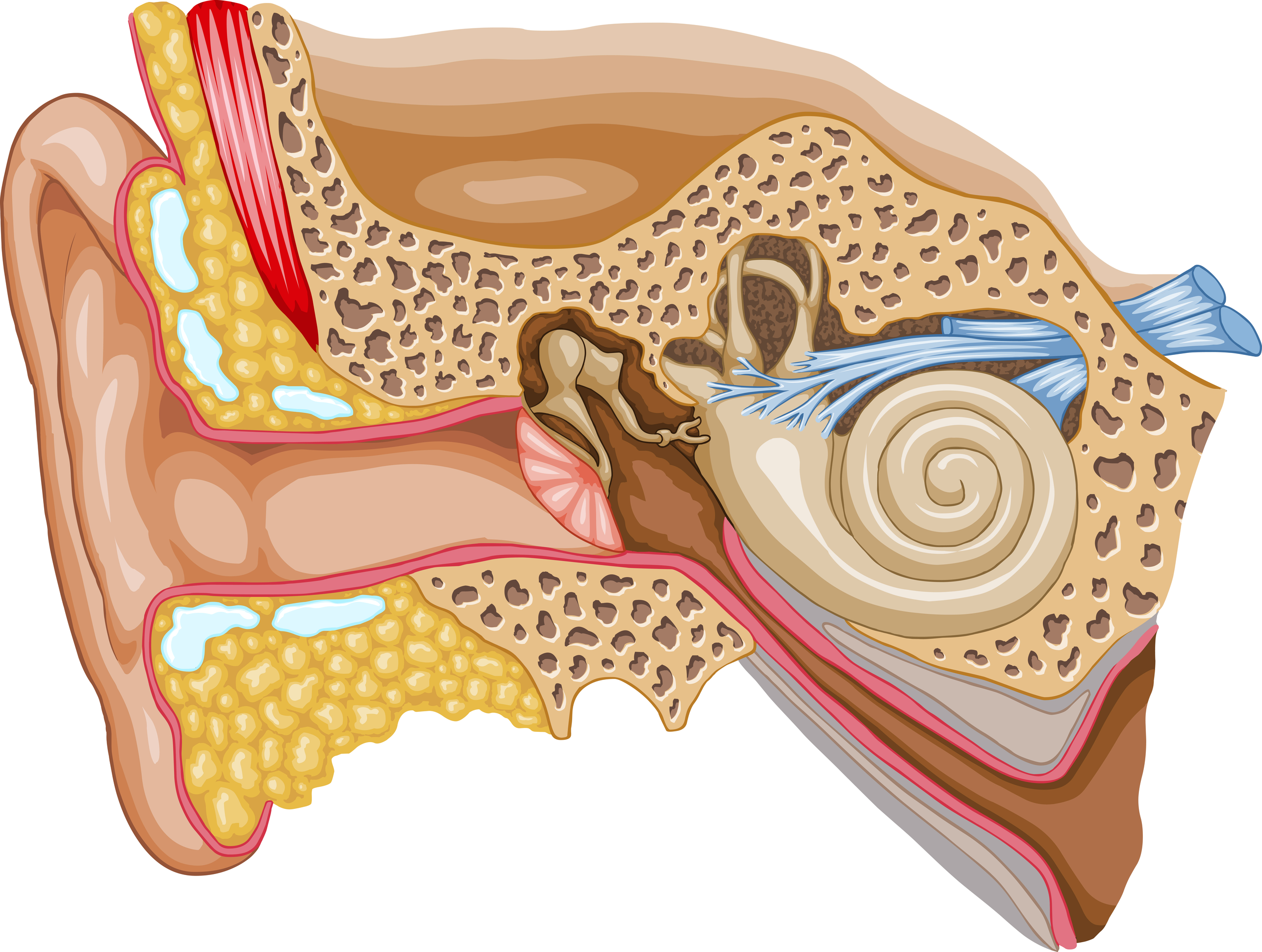
The ear is divided into three sections: outer, middle, and inner ear. Sound waves travel through the ear canal of the outer ear and strike the eardrum, which causes three, tiny middle-ear bones to vibrate. These vibrations move tiny hairs in the snail-shaped structure of the inner ear called the cochlea. The hairs transform sound-wave vibrations into electrical signals that travel along the cochlear nerve to the brain, where they are translated into familiar sounds.
However, many conditions can interfere with this process. The ear is sensitive to movement, changes in temperature, diseases, and air and water pressure. The following is information about common ear conditions you may experience.
EAR INFECTIONS
Ear infections often occur when one of the Eustachian tubes that connect the ear to the back of the throat becomes swollen and fluid builds up in your middle ear, the section just behind the eardrum. Bacteria or a virus can also cause an infection of the middle ear. Such infections can be quite painful because of the inflammatory response and pressure from fluid build up. These infections can be either acute or chronic. Acute infections are painful, but short in duration. Chronic infections either do not clear up, or recur many times, causing permanent damage to the middle and inner ear.
Forms
Infections occur either in the outer or middle ear. Outer ear infections are usually from swimmers ear, where water from swimming (or bathing) has introduced bacteria. Middle ear infections have three categories: acute otitis media, otitis media with effusion, and chronic suppurative otitis media.
Causes
The causes of the three types of middle ear infection include:
- Acute otitis media: A bacterial or viral infection of the middle ear
- Otitis media with effusion: The presence of fluid in the middle ear without the infectious symptoms of acute otitis media. Most often, this occurs after an acute infection has cleared, but the fluid persists.
- Chronic suppurative otitis media: Causes drainage from the ear for six weeks or longer.
Other causes of infection include:
- Allergies
- Sinus infections
- Colds
- Excess mucus
- Infected or swollen adenoids
- Tobacco smoke
Ear Infection Symptoms: Ear infection symptoms include itching, swelling, pain, and a yellow discharge from the ear. You may also have hearing loss from the inflammation or discharge, which can block the ear canal. In time, your ear may become painful to touch and infection may spread to other ear structures. Middle ear infections symptoms include the sudden development of earache, pain, fever, and feeling sick and irritable. These symptoms might persist, or come and go.
Screening to Diagnose
To check for infections, your doctor inspects your ear with a viewing tool called an otoscope, which has a light and magnifying lens.
Treatments
Most mild ear infections clear up on their own. Applying a warm cloth can help reduce pain and swelling. If medication is needed, antibiotics in the form of eardrops help clear up bacterial infections, antifungal drugs kill fungus, and anti-inflammatory drugs reduce swelling. If antibiotics fail, your doctor may suggest tubes be inserted through the eardrum to drain the fluid. Surgery may be recommended if the problem persists.
Prevention
The best way to prevent outer ear infections is to keep water out of the canal, even when showering. Place a ball of cotton covered with a layer of petroleum jelly into your ears. After bathing, remove the cotton and air out the ear canals. Also, use earplugs when swimming.
Since acute otitis media occurs most often in children, and can recur, you should look for other underlying causes such as environmental allergens, food allergies, immune deficiencies, enlarged adenoids, chronic sinusitis, and exposure to tobacco smoke. Keeping immunizations up-to-date also can help.
TINNITUS
More than 50 million Americans have tinnitus which causes sufferers to perceive noise in one or both ears when no external sound exists. The noise can occur intermittently or persistently. It can interfere with sleep and concentration, and has been linked with stress and depression. Tinnitus usually can be traced to a problem with the inner ear, but sometimes the underlying cause is less clear. However, tinnitus often improves over time, and you also may be able to manage the problem by altering your reaction to it.
Forms
There are three types of tinnitus.
- Tonal tinnitus is often called “ringing in the ears.” This type produces a continuous sound, like a single note played over and over.
- Pulsatile tinnitus is when the sounds are intermittent, continuous, or pulsating in time with the heartbeat.
- Musical Tinnitus is the perception of music or singing in a constant loop, and is the most rare.
Causes
Tinnitus sounds often originate from the inner ear. As you age, tiny sensory hair cells in the inner ear die off, or are damaged. This process may be accelerated by exposure to loud noises, poor cardiovascular health, and some medications, including aspirin and acetaminophen, diuretics, and antibiotics. Middle ear infections, and rare conditions that cause the ear bones to harden, also may trigger tinnitus.
Certain non-auditory conditions and lifestyle factors also are associated with tinnitus. For example, temporomandibular joint (TMJ) disorders (which affect the hinged joint attaching the jaw to the skull), depression, anxiety, insomnia, and muscular stress and fatigue. Tinnitus also can result from a head or neck injury.
Risk Factors
While anyone can experience tinnitus, these factors may increase your risk:
- As you age, the number of functioning nerve fibers in your ears decline, which can lead to hearing problems associated with tinnitus.
- Gender. Men are more likely to experience tinnitus than women.
- Loud noises. Prolonged exposure can damage the sensory hair cells in your ears that transmit sound to your brain.
- Cardiovascular problems. Conditions that affect your blood flow, such as high blood pressure or narrowed arteries, can increase your risk.
- Smoking
Symptoms
Tinnitus is most often described as ringing in the ears, although some people report hearing sounds like buzzing, hissing, roaring, clicking, or chirping.
Screening to Diagnose
Screening involves a thorough medical examination of the outer and inner ear, and a review of your medical history. Your doctor then may use one or more of the following tests:
- Hearing (audiological) exam. You will sit in a soundproof room wearing earphones through which specific sounds are played into one ear at a time. You indicate when you can hear the sound, and your results are compared with results considered normal for your age. About 90 percent of those who experience tinnitus also suffer from hearing loss.
- You are asked you to move your eyes, clench and unclench your jaw, and/or move your neck, arms, and legs in certain directions. If your tinnitus changes or worsens when you do these, it may help to identify an underlying problem.
- Imaging tests. Depending on the suspected cause of your tinnitus, you may need imaging tests, such as computed tomography (CT) scan or magnetic resonance imaging (MRI) scan.
Treatment
Even if a specific cause is identified, addressing it may or may not eliminate the problem. If not, one or more of these strategies may offer relief.
- Identify and avoid triggers. Pinpoint anything that exacerbates the symptoms—for example, drinking caffeinated beverages, taking particular medications, or exposure to noise.
- Use hearing aids. If you have hearing loss, wearing a hearing aid may reduce tinnitus by reintroducing ambient sounds to mask it.
- Change your reaction. Cognitive behavioral therapy (CBT) can help recognize negative behaviors and thought patterns related to your tinnitus, so you may consciously alter them to reduce your distress from the noises. A similar approach is tinnitus-retraining therapy, which uses counseling and sound therapy to train your brain to ignore the tinnitus.
- Seek out other sounds. Sound therapy uses a constant, neutral sound to distract you from the noise of your tinnitus. Examples include tuning a radio to static sounds, or using a sound machines that plays “white noise” or relaxing nature sounds.
Prevention
You can take some precautions to protect yourself from certain kinds of tinnitus.
- Use hearing protection. Always wear over-the-ear protection when exposed to loud noises or machinery like lawn equipment, music, crowds, and firearms.
- Improve cardiovascular health. Regular exercise and eating right can keep blood vessels healthy and reduce risk of tinnitus linked to blood vessel disorders.
WHAT IS VERTIGO?
Vertigo is a sensation where you feel as if you are spinning or that the world around you is spinning. It is caused by vestibular (balance) system disorders that originates in the inner ear where balance is regulated.
Forms
There are three types of vertigo:
- Benign paroxysmal positional vertigo (BPPV). This occurs when tiny calcium crystals in the utricle (one of the structures of the inner ear) break loose and stimulate sensory hair cells in the inner ear. This can result in brief spells of intense spinning that are triggered by turning over in bed, bending down, or looking up.
- Vestibular neuritis (acute labyrinthitis). This is caused by a viral infection of the inner ear and cochlea, and often develops after a cold or the flu. It manifests as a sudden, unexpected attack of vertigo that can last from a few days to a few weeks.
- Meniere’s disease. A problem related to sodium and fluid balance in the ear. The onset may be sudden, and may last for several hours, causing nausea, and vomiting.
Causes
Certain medications or taking more than prescribed or mixing drugs with alcohol may also trigger vertigo. A head or neck injury, migraine headaches, or stroke are other common causes.
Symptoms
Symptoms can last a few minutes to a few hours or more and may come and go. People with vertigo often describe it as feeling like they are:
- Spinning
- Tilting
- Swaying
- Unbalanced
- Pulled in one direction
Other symptoms that may accompany vertigo include:
- Lightheadedness or dizziness
- Nausea
- Abnormal or jerking eye movements
- Headache
- Sweating
Screening to Diagnose
Screening begins with a physical exam where you describe your first episode, the character of the vertigo, what you were doing when it began, and the frequency and severity of other episodes. The exam also helps identify nystagmus (a repetitive, abnormal eye movement) and any abnormalities in gait and balance that may contribute to your vertigo.
Several diagnostics tests can help identify possible causes. For instance, an audiogram (hearing test) and electronystagmography (ENG) record the function of your hearing and balance systems. An MRI can rule out tumor, stroke, or multiple sclerosis.
Treatment
Sometimes vertigo goes away on its own as the brain is able to adopt to some inner ear changes in order to maintain balance. It treatment is needed, the following options are often used:
Vestibular rehabilitation. Physical therapy is used to correct any issues in your vestibular system, such as problems with balance, neck motion, and visual stability, and gait. The types of therapy often used are posture and balance training, stretching routines, and neck motion exercises.
Epley maneuver. This is used to treat BVVP by helping to dislodge calcium crystal debris. A doctor or physical therapist performs the 10 to 15-minute session. It works like this:
- In a seated position, your head is turned 45 degrees horizontally toward the affected ear.
- You are then tilted backward until you are horizontal with your head kept in place at a hanging, 45-degree angle. An attack of vertigo will likely occur as the calcium crystal debris moves toward the apex of the canal. You stay in this position for 30 seconds or until the vertigo stops.
- The doctor or therapist then turns your head 90 degrees toward the unaffected ear. He or she then rolls you onto the side of the unaffected ear, so you look at the floor. The debris should move in the canal again, and trigger another vertigo episode. Again, you are held here for 30 seconds, or until the vertigo stops.
Prevention
Besides seeking necessary care and treatment, review your medications with your doctor to determine if any contribute to attacks, and avoid or restrict alcohol intake as it can cause or worsen dizziness.
HEARING LOSS
Most people experience some hearing loss as they age. For some, it can begin in their 50s, while for others is does not happen until their 70s or 80s.
Forms
Hearing loss is often classified by degrees: mild, moderate, severe, and profound.
- Mild: It is difficult to follow conversation in the presence of background noise.
- Moderate: You need people to repeat themselves during in-person conversations on a regular basis.
- Severe: It is almost impossible to follow a conversation without a hearing aid.
- Profound: You cannot hear other people speaking, unless they are quite loud, and you cannot understand speech without a hearing aid or cochlear implant.
Causes
The most common cause of hearing loss is advanced age, also called presbycusis. As people age, cochlear hair cells in the inner ear designed to pick up sound waves become damaged or die. These cells do not regenerate.
Another cause of poor hearing is repeated exposure to loud noise over many years. Head or ear trauma also can lead to diminished hearing, as can poor blood flow to the inner ear, which may be caused by cardiovascular disease and/or diabetes. Certain medications have been known to aggravate hearing loss, such as antibiotics, diuretics, chemotherapy drugs, salicylates, and nonsteroidal anti-inflammatory drugs like ibuprofen (Advil) and naproxen (Aleve).
Symptoms
Here is a list of some of the common symptoms:
- Certain sounds are difficult to decipher, such as high-pitched children’s and female voices, and the sounds of certain constants like “S” and “F.”
- Difficulty hearing above background noise
- Trouble following a conversation when multiple people speak, or misunderstanding what people say
- Perception that people are not speaking clearly or mumbling
- Asking people to repeat themselves
Screening to Diagnose
There are several methods to diagnose possible hearing loss.
- Physical exam. Your doctor examines your ears with a lighted instrument called an otoscope to look for earwax buildup, inflammation, and fluids from an infection, or possible obstruction in the ear canal.
- General screening test. You cover one ear at a time to see how well you hear words spoken at various volumes and how you respond to other sounds.
- Tuning fork tests. You listen to the vibrating sounds of two-pronged instruments. This test can also help determine if hearing loss is caused by damage to the vibrating parts of your middle ear, nerves of your inner ear, or both.
- Audiometer tests. Conducted by an audiologist, this involves wearing earphones and listening to a range of sounds at differing volumes in one ear at a time and then both ears simultaneously. You indicate each time you hear a sound. This helps to identify at which sound level you have trouble registering.
- Imaging tests. A CT or MRI scan may be done if an injury or tumor is suspected.
- Auditory brain stem response (ABR) test. This is used to test nerve pathways in the brain if your doctor suspects an acoustic neuroma or other nerve problem.
Treatments/Surgery
Treatment options depend on the cause of hearing loss and its severity. For reversible hearing loss, common treatments include antibiotics for infection, earwax removal, and necessary medication or even surgery to address an injury.
For permanent hearing loss caused by age and noise exposure, you can turn to hearing aids or cochlear implants. A hearing aid is a small electronic device you wear in or behind your ear that amplifies sound and speech so they are easier to understand. Surgery is used for cochlear implants. The implant sends impulses to your auditory nerve, which carries signals to your brain. This is often used for severe hearing loss in one or both ears.
Prevention
The best ways to protect yourself is to avoid or limit your exposure to noisy environments, wear earplugs when exposed to high-noise levels such as when moving the lawn, and have regular check-ups with an audiologist. Certain lifestyle habits can impede blood flow to the ear and affect hearing, such as smoking, high blood pressure, and diabetes. Take measures to lower your risk of these conditions by quitting smoking, adopting a healthy diet, and increasing the amount, you exercise.
III. THE NOSE
Overview
The nose performs three functions: it detects and distinguishes smells, helps to keep foreign matter out of your lungs, and warms and humidifies the air you breathe. Buried in the inner lining of the nose are millions of nerve endings that create electrical impulses when they encounter a scent. These impulses travel up the olfactory nerve to the brain, where they are recognized as specific smells. Here is a look at some of the common problems that affect the nose and your sense of smell.
WHAT IS SINUSITIS?
Sinusitis, also known as sinus infection, is an inflammation of the sinus tissue. When your sinuses become blocked with fluid, bacteria, viruses and fungi can grow and lead to an infection.
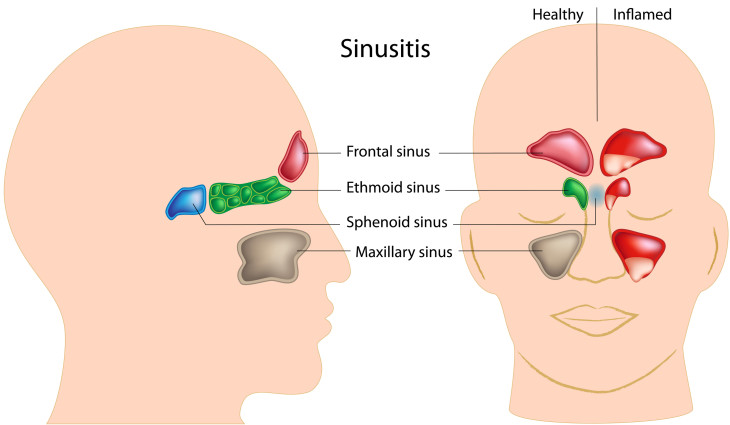
The sinuses main function is to produce a mucus that moisturizes the inside of the nose. This mucus layer protects the nose from pollutants, micro-organisms, dust and dirt. Click the image to expand view.
Forms
There are several types of sinusitis. The main differences are the severity and length of flare-ups. They include:
- Acute sinusitis: About four weeks or less.
- Subacute sinusitis: Four to eight weeks.
- Chronic sinusitis: Longer than eight weeks.
- Recurrent sinusitis: Occur many times a year.
Causes
Conditions that can cause sinusitis include bacteria, fungi, or viruses related to the common cold, allergic rhinitis (swelling of the lining of the nose caused by exposure to allergens and smoke), nasal polyps (small growths in the lining of the nose), or a deviated septum (a shift in the nasal cavity that is often hereditary).
Symptoms
The main symptoms of acute sinusitis, the most common type of sinusitis, include one or more of the following:
- Facial pain
- Nasal stuffiness
- Yellow and/or green nasal discharge
- Headache
- Cough or congestion
- Fever
- Fatigue
- Loss of smell
Screening to Diagnose
A physical exam can check if your sinuses are inflamed, and if you have nasal polyps. Other tests may include a nasal endoscopy—a tube-like instrument with tiny lights and cameras that examines the interior of your nose and sinus drainage areas—as well as X-rays, allergy and blood tests, and a CT scan.
Treatments
Over-the-counter decongestants, antifungal medicine, and nonprescription decongestant nasal drops or sprays are often effective at controlling mild symptoms, but should only be used for a few days. Antibiotics are prescribed for 10 to 14 days for more severe cases. For chronic sinusitis, oral steroids might be prescribed to reduce inflammation. A vaporizer or inhaling steam from a pan of boiling water also may alleviate congestion, and warm compresses help to relieve nasal and sinus pain. Antihistamines may be recommended for the treatment of infections caused by allergies.
Prevention
The best ways to prevent sinusitis is to reduce exposure to your triggers. For instance, protect yourself from bacteria, viruses, and fungus by keeping your home and work environment clean, smoke-free, and dry. Wash your hands regularly, especially during cold and flu season.
Another option is to flush your nasal passages with a store-bought or home-made solution of hypertonic saline (salt water), which can improve reduce nasal swelling and remove debris and allergens.
NASAL ALLERGY
Nasal allergies are an inflammatory reaction to certain environmental substances, such as dust mites, mold, animal hair, grass, or pollens.
Causes
Pollen is the most common cause of allergens, especially during the spring and fall when tree, flower, grass, and weed pollen are at their greatest density in the environment.
Risk Factors
Allergies can happen to anyone, but your risk is higher if you have a family history of allergies. Environmental pollutants also play a role, such as smoke, chemicals, and perfumes.
Symptoms
The natural chemical histamine is released when your body encounters an allergen in order to defend itself. This is what causes the typical symptoms, such as:
- Constant sneezing
- Runny and/or stuffy nose
- Coughing
- Sore or scratchy throat
- Itchy and watery eyes
- Headaches
- Facial pain
- Extreme fatigue
Screening to Diagnose
Isolating the source of your allergy can often be done through a physical exam. However, you may need other tests to help isolate the allergen and determine the best treatment and preventative options. The two most used are the skin prick and allergy blood tests.
- Skin prick. A doctor places a variety of substances onto your skin to see how your body reacts to each one. A small red bump appears if you are allergic to a substance.
- Blood test. This measures the amount of immunoglobin E (IgE) antibodies to particular allergens that are present in your blood.
Treatments
There are various ways to treat nasal allergies.
- Antihistamines. They prevent this condition by blocking histamine formation in the body. Some over-the-counter (OTC) versions work fine, but check with your doctor before.
- Decongestants. OTC decongestants used over a short period of time can relieve stuffy nose and sinus pressure. Again, check with your doctor, especially if you have high blood pressure or an enlarged prostate.
- Eye drops and nasal sprays. They relieve itchiness and other symptoms related to allergies.
- Immunotherapy (allergy shots). You can use this approach in conjunction with medications to control your symptoms. Over time, the injections lower your immune response to specific allergens.
Prevention
The best way to prevent symptoms is to manage your allergies. For instance, begin medications before seasonal allergies attack, stay indoors when pollen counts are high, and take special care to keep your home free of pet hair, dust, and mold.
IV.THE THROAT
Overview
Your throat houses the larynx (voice box) and vocal cords needed for speech, it is lined with immune system cells that guard against incoming germs, and it provides a passageway for air to flow into your lungs. However, just as with your ears and nose, it is vulnerable to certain problems.

Say aaaahh. Your doctor can tell what throat condition you’re experiencing by looking at the tissues and structures inside your mouth.
LARYNGITIS
Laryngitis is an inflammation of your larynx from overuse, irritation, or infection.
The larynx is where your vocal cords are located. They consist of two folds of mucous membrane that cover muscle and cartilage. When laryngitis strikes, your vocal cords become inflamed or irritated and this swelling causes distortion of the sounds produced by air passing over them. As a result, your voice sounds hoarse, and is some cases almost undetectable.
Most cases of laryngitis are triggered by a temporary viral infection or vocal strain and improve on their own. However, persistent hoarseness can sometimes signal a more serious underlying medical condition.
Forms
Laryngitis may be short-lived (acute) or long lasting (chronic), which means it can last for longer than three weeks.
Causes
Viral infections similar to those that cause a cold, and vocal strain from overuse or yelling, are the most common causes. Others include:
- Exposure to irritants, such as chemical fumes, allergens or smoke.
- Gastroesophageal reflux disease (GERD)
- Chronic sinusitis
- Excessive alcohol use
- Smoking
- Vocal cord paralysis resulting from injury, stroke, or a tumor
- Age-related bowing of the vocal cords
Symptoms
In most cases, symptoms last for a few weeks at the most. They include:
- Hoarseness
- Weak voice or voice loss
- Tickling sensation or throat rawness of your throat
- Sore or dry throat
- Dry cough
Screening to Diagnose
If you have chronic laryngitis, your doctor will examine your vocal cords, and may refer you to an ear, nose and throat specialist (otorhinolaryngologist) for evaluation.
A laryngoscopy is an instrument that uses a light and a tiny mirror to look into the back of your throat. Another diagnostic tool sometimes used is a fiber-optic laryngoscopy. Here, a thin, flexible tube with a tiny camera and light is inserted through your nose or mouth and into the back of your throat. This allows your doctor to watch the motion of your vocal cords as you speak. If any polyps or suspicious growths are detected, a biopsy will be taken for analysis.
Treatment/Surgery
Acute laryngitis often gets better on its own with rest after a week or so. For chronic laryngitis, the goal is to treat the underlying causes, such as heartburn, smoking, or alcohol use. If you have a bacterial infection, your doctor may recommend an antibiotic. Surgery may be required to remove any polyps.
Prevention
Curbing the use of your voice, and providing plenty of rest for your vocal cords will help. Eliminating or reducing your exposure to smoke and alcohol can stop irritation. Other strategies include:
- Drink plenty of water. Fluids help make the mucus in your throat easier to clear.
- Avoid eating spicy foods. They can cause stomach acid to move into the throat or esophagus, which can cause heartburn.
- Stop clearing your throat. This causes an abnormal vibration of your vocal cords and can increase swelling.
- Wash your hands often. This help protect against the spread of germs that cause colds/
DYSPHAGIA
Difficulty swallowing, called dysphagia, means it takes extra effort to move food or liquid from your mouth to your stomach. Dysphagia can also cause pain and in some cases make swallowing almost impossible. It can occur at any age, but is more common in older adults. If persistent, dysphagia may indicate a serious medical condition that requires treatment.
FORMS
Dysphagia falls into one of the following categories:
- Esophageal dysphagia: The sensation of food sticking or getting hung up in the base of your throat or in your chest after you have swallowed.
- Oropharyngeal dysphagia: This occurs when certain conditions weaken your throat muscles, and makes it difficult to move food from your mouth into your throat and esophagus. You may choke, gag, or cough when you try to swallow or have the sensation of food or fluids going down your windpipe or up your nose.
CAUSES
Some of the causes of esophageal dysphagia include the following:
- This is when your lower esophageal muscle (sphincter) does not relax properly to let food enter your stomach.
- Diffuse spasm. This causes intense contractions of the esophagus, often after you swallow.
- Esophageal stricture. A narrowed esophagus can trap large pieces of food. Sometimes tumors or scar tissue from gastroesophageal reflux disease (GERD) can cause this narrowing.
- Esophageal tumors. Difficulty swallowing tends to get worse when they are present.
- Foreign bodies. Sometimes food or another object can partially block your throat or esophagus.
- Radiation therapy. This cancer treatment can lead to inflammation and scarring of the esophagus.
Some causes of oropharyngeal dysphagia include:
- Neurological disorders. Examples: multiple sclerosis, muscular dystrophy and Parkinson’s disease.
- Neurological damage. A stroke or brain or spinal cord injury, can affect your ability to swallow.
SYMPTOMS
Besides the difficulty and pain associated with trying to swallow, sufferers may also experience these symptoms:
- Having the sensation of food stuck in your throat or chest
- Drooling
- Being hoarse
- Bringing food back up (regurgitation)
- Frequent heartburn
- Unexpected weight loss
- Coughing or gagging when swallowing
Screening to Diagnose:
Your doctor will likely perform a physical examination and may use a variety of tests to determine the cause of your swallowing problem. These tests may include:
- Barium X-ray. This helps see changes in the shape of your esophagus and review muscular activity. You first drinking a barium solution to coats your esophagus, which improves the X-ray image.
- Dynamic swallowing study. You swallow barium-coated foods of different consistencies. This provides an image of these foods as they travel through your mouth and down your throat, and may show problems in the coordination of your mouth and throat muscles when you swallow.
- A visual examination of your esophagus using a thin, flexible lighted instrument, which is passed down your throat in order to view your esophagus.
- Fiber-optic endoscopic swallowing evaluation (FEES). As you tyr to swallow, your throat is examined with a special camera (endoscope) and lighted tube.
- Esophageal muscle test (manometry). A tube is inserted into your esophagus and then connected to a pressure recorder. As you swallow, the muscle contractions of your esophagus are measured.
- Imaging scans. These may include a CT scan, an MRI scan, or a positron emission tomography (PET) scan.
Treatments/Surgery
Treatment for dysphagia depends on the type or cause of your swallowing disorder. If you have oropharyngeal dysphagia, you may be referred to a speech or swallowing therapist who may suggest special exercises to help coordinate your swallowing muscles or improve your swallowing reflex. Another technique is to teach you how to place food in your mouth or position your body and head in certain positions to encourage normal swallowing.
Treatment approaches for esophageal dysphagia may include:
- Esophageal dilation. For a tight esophageal sphincter, an endoscope with a special balloon attached is inserted down your esophagus in order to gently stretch and expand the sphincter’s width.
- Surgery. For an esophageal tumor, you may likely require surgery to clear your esophageal path.
- Medications. Drugs to help reduce stomach acid can help if you have problems swallowing because of GERD.
Prevention
Although swallowing difficulties cannot be 100 percent prevented, you can reduce your risk by cutting food into smaller pieces, eating slower, and avoiding certain foods that are tough to swallow. Early detection and effective treatment of GERD also can lower your risk.
 Hearing Aids Extend Longevity
Hearing Aids Extend Longevity  How to Fix a Droopy Eyelid
How to Fix a Droopy Eyelid