Bladder Control Begins with Behavior Modification
A board-certified urogynecologist helps us understand the best steps to treating bladder control in overcoming urinary incontinence.
If you’ve experienced urinary incontinence, you know all about bladder control—or a lack thereof. It’s when you leak urine involuntarily while coughing or sneezing and/or you are unable to get to the bathroom before urine is released.
A study published in Reviews in Urology stated that incontinence can become a problem around menopause in women, and that it can rapidly increase between the ages of 70 and 80 for both men and women. Women tend to deal more with mixed incontinence (incontinence caused by stress and by urge; more on that below), whereas men usually have urge incontinence.
WHAT IS BLADDER CONTROL?
Loss of ladder control is not just leakage. It can also be diagnosed because you’re urinating more than often than before and it’s interfering with your life; you get up to use the bathroom two or more times a night; you’ve experienced bed-wetting; or you’re experiencing painful urination. These habits are not normal, and they should be addressed by a physician.
Urinary incontinence is not a disease. It can be a symptom of another problem, such as a urinary tract infection, constipation, neurological diseases, diabetes, or an anatomical abnormality (a pelvic organ prolapse, for example). It also can be a side effect from a medication (diuretics, for instance) or even a symptom of drinking too much water.
According to the U.S. National Library of Medicine, twice as many women experience bladder-control problems as men (see sidebar), so we’ll focus here on female incontinence. However, universal causes of bladder-control issues include obesity, weakness in the pelvic floor muscles, birth defects, chronic coughing, genetics, aging, and physical inactivity.
BLADDER CONTROL IN MEN
Besides the universal causes of incontinence listed in our story, men can have problems with bladder control due to an enlarged prostate or prostate cancer. The National Institute of Health estimates 11 to 34 percent of men deal with incontinence.
What Causes Bladder Control Problems?
It’s important to know the cause of your bladder control problems. “Incontinence can occur due to neurological issues, spinal-cord injuries, and even compressed disks,” says Samuel S. Badalian, MD, PhD, ScD, Director of The Gynecology-Urogynecology Center in Syracuse, N.Y. “It’s so important to see a medical provider who knows how to do the proper diagnostic testing to rule-out other problems that may be causing the incontinence, such as pelvic prolapse.”
With a prolapse, the pelvic organs—bladder, uterus, rectum—drop out of place, bulging into the vagina. “Weakened pelvic-floor muscles can result in prolapse as well as urinary incontinence,” says Dr. Badalian, who is board-certified in both gynecology and Female Pelvic Medicine and Reconstructive Surgery.
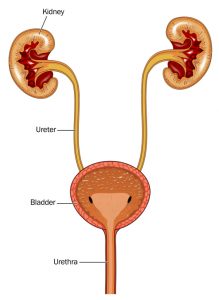
This diagram shows the relationship of the bladder to the kidneys. Loss of bladder control can result in multiple types of urinary incontinence, including functional incontinence and stress incontinence
Women, not surprisingly, can have urinary incontinence due to vaginal childbirth, which can result in eventual pelvic prolapse. Vaginal laxity, or looseness, is an early warning sign of prolapse.
A 2012 study from the University of Gothenburg found that women are nearly three times more likely to experience urinary incontinence 10 years following a vaginal delivery than after a caesarean section. A 2016 study from the University of Helsinki was slightly more conservative, putting the risk at double.
One of the early signs that the pelvic-floor muscles are weakening is vaginal relaxation. “Vaginal laxity or ‘looseness’ is common in our urogynecology service at a prevalence of 24 percent,” reported a study published in the May 2018 edition of the International Urogynecology Journal. The study concluded that vaginal laxity may be considered an early symptom of prolapse.
Types of Urinary Incontinence
The type of urinary incontinence you’re experiencing can make a difference in the therapy your doctor prescribes for bladder control.
CHOOSING A TRAINED PHYSICIAN
The medical specialty Female Pelvic Medicine and Reconstructive Surgery (FPMRS) began in 2013, giving women the option of seeking a physician with advanced training in female pelvic-organ prolapse and bladder-control issues. You can find these physicians through the American Urogynecologic Society and American Urological Association. Men routinely see a urologist, who should be board-certified through the American Board of Urology (some urologists are also board-certified in FPMRS, too).
- Functional incontinence: This is the term for incontinence that occurs due to a person’s inability to get to the bathroom. Patients with Parkinson’s disease, cerebral palsy, dementia, severe depression (they simply don’t care) may have functional incontinence. So too to those with an inability to express the need to void or the inability to remove clothing in order to void, or who have no suitable bathroom available (one that’s in a location that’s difficult to reach or too small to accommodate a wheelchair, for example).
- Mixed incontinence: A combination of urge and stress incontinence (see below).
- Overactive bladder: In this condition, the bladder begins to contract involuntarily. It often occurs in patients with diabetes, Parkinson’s disease, multiple sclerosis, bladder stones, urinary-tract infections, neurological conditions, and certain medications.
- Stress incontinence: With stress incontinence, urine leaks out when you cough, sneeze, lift something heavy, laugh hard, running—anything that puts physical stresses or pressures your bladder.
- Total incontinence: This is constant urinary leakage.
- Transient incontinence: Transient, or temporary, incontinence usually occurs due to side effects of medications or an illness.
- Urge incontinence: In urge incontinence, you experience an all-of-the-sudden need to get to a bathroom. Urine may leak during your run to the facility, and you cannot stop it.

If you have bladder control issues, you can relate to this restroom sign.
Loss of Bladder Control: Diagnostics
To begin the process of diagnosing bladder control problems, your physician will take a complete history and do a thorough examination, procedures usually done in the physician’s office. Depending upon the suspected cause, you may be asked to keep a voiding or bladder diary.
In this diary, you list things like how much liquid you consumed, what you drank, and when you consumed it. You will also keep track of when you urinated and may be asked to estimate the quantity of urine (small, medium, large), how strong the urge was, and what you were doing at the time. Your answers will help your physician determine whether you’re experiencing urge incontinence. Your physician will likely do a urinalysis, looking for possible infections and blood in your urine.
Plus, you may be asked to do urodynamics testing, which can tell the physician how well your bladder, sphincters, and urethra are storing and releasing urine. The doctor will learn whether your bladder is releasing urine on its own, the speed with which urine is released, how strong the flow of urine is, whether you can physically stop the flow of urine, and the amount of urine you’re producing from a full bladder. He can check the muscle activity in the area, too. This information helps your doctor pinpoint more closely the cause of incontinence.
A cystoscopy, where the surgeon puts a catheter into your bladder to examine it and its lining for abnormalities, may be needed, especially if you’re seeing blood in your urine.
Correcting Bladder Control Problems with Behavior Modification
The treatment your physician chooses depends somewhat upon the cause. Certain treatments are simply changes in your own behavior. “Behavior modification is an important part of treating incontinence,” says Dr. Badalian.
Besides the bladder diary mentioned earlier, your physician likely will instruct you to make these types of lifestyle changes:
- Avoid foods and beverages high in caffeine, which is a stimulant.
- Change your diet to try to reduce common bladder irritants, like spicy foods, citrus fruit, tomato products, dairy, and added sugar.
- Cut back on alcohol.
- Do not drink carbonated beverages.
- Exercise.
- Head to the bathroom before you feel the urge to urinate, even timing yourself to ensure you don’t forget (this is called “bladder training”).
- Lose weight.
- Practice regular Kegel exercises, which can strengthen the pelvic-floor muscles and sphincters to help you regain control.
- Quit smoking.
- And, most important, drink only when you’re truly thirsty.
Regarding that last point, physicians often see a connection between the amount of liquid a person drinks and their bladder habits. The oft-touted “keep yourself hydrated” mantra doesn’t necessarily apply to everyone.
“Drink when you’re thirsty,” says Dr. Badalian. “I have patients who come in and say they have been told to drink huge amounts of water every day. Some have even told me they believe all that water is physically cleansing. This is simply not the case. When you’re thirsty, drink a glass of water. If you’re not thirsty, don’t drink water.”
The norm for most people: six to eight 8-ounce glasses of water.
The instructions to exercise and lose weight may sound like “been there” reasons for physical problems—don’t you hear that for like everything you discuss with your doctor? But a study from the University of Jyväskylä, published in 2017 in PLOS One, showed that urinary incontinence symptoms in middle-aged woman are linked to lower levels of exercise. It’s a chicken-and-egg situation, though. The study found that involuntary urinary incontinence symptoms can discourage sufferers from partaking in exercise, but exercise can ease symptoms by reducing obesity (obesity increases pressure on the urethra) and strengthening pelvic floor muscles, which help with bladder control.
Bladder Control: Kegel Exercises
While behavior modification and the BTL EMSella (see sidebar) top the list of non-invasive, non-drug solutions to incontinence and bladder control, physicians have an array of therapies from which to choose.
When the deterioration of the pelvic-floor muscles is noted early enough, physicians often recommend that women do regular Kegel exercises. You can do Kegel exercises virtually anytime and anywhere. While this therapy can work, many women struggle with remembering to do the exercises and worry about whether they are contracting the right muscles.
“To identify the muscles, when you are urinating, stop the stream—these are the muscles that need to be strengthened,” advises Bilal Chughtai, MD, a urologist at Weill Cornell Medicine. “However, don’t do the exercises when you are urinating.
“A Kegel exercise consists of contracting (squeezing) the muscles for several seconds and then relaxing them,” Dr. Chughtai says. “Do at least 20 Kegels every day and continue to do them daily; you have to do them regularly to get results.”
INCONTINENCE AND BLADDER CONTROL: NEWEST THERAPY
Released in 2018, the non-surgical, non-drug BTL EMSella has a 95 percent success rate of curing a woman’s urinary incontinence or vaginal laxity, just by her sitting, fully clothed, on a chair for six 30-minute sessions. The effects last a year, with an annual one-session follow-up.
The FDA-cleared BTL EMSella uses high-intensity, focused electromagnetic technology to stimulate the deep pelvic-floor muscles, which brings back neuromuscular control to the urethral sphincter and keeps the pelvic organs in place. For women who prefer to avoid drugs and surgery, the BTL EMSella may be the answer.
The BTL EMSella delivers approximately 11,000 muscle contractions, or Kegels, in 28 minutes. These sessions “re-educate” the pelvic floor muscles, eliminating vaginal looseness and strengthening the muscles that support bladder and uterus.
Many medications address bladder control and urinary incontinence, including:
- Oxybutynin (Ditropan XL)Tolterodine (Detrol)
- Darifenacin (Enablex)
- Fesoterodine (Toviaz)
- Solifenacin (Vesicare)
- Trospium (Santura)
- Mirabegron (Myrbetrq)
- Tamsulosin (Flomax)
These medications relax the bladder muscles, targeting urge incontinence and overactive bladder. Myrbetrq, which is a new class of medication (alpha adrenergic), also increases the amount of urine the bladder can hold.
Ian Milsom, Professor of Gynecology and Obstetrics at the Sahlgrenska Academy and Head of the Gothenburg Continence Research Center (GCRC), questions the use of medications, saying he finds it remarkable, including from a financial perspective, that these antimuscarinic drugs aren’t helping even half of all patients.
“The results don’t look good at all considering the cost in billions that these drugs incur on health-care systems,” according to Milsom. “In contrast, surgery, on the other hand, has become simpler and more effective and is delivering strong results even in the long term.”
Milson’s study, from the University of Gothenburg, was published in BMC Medicine in March 2017. Findings showed that surgery was successful in 82 percent of bladder control cases. Pelvic floor exercises ranked second, with 53 percent, followed by drug treatment, with 49 percent.
Dr. Badalian believes the BTL EMSella, which arrived on the scene after the study referenced above, is the future, with its high effectiveness rating and the fact that it could eliminate both the high cost of surgery and recovery time for the patient. The therapy is currently available in a limited number of urogynecology offices.
SOURCES & RESOURCES
For related reading, please visit these posts:
- Don’t Suffer in Silence: Report Urine Leakage to Your Doctor
- Natural Remedies for Overactive Bladder: Herbs, Bladder Training, and More
- Most Common Health Problems in Elderly People
- UTIs: How to Prevent and Treat Urinary Tract Infections
- Bladder Cancer Symptoms: Seek an Evaluation for Early Detection
Types of Bladder Control Surgeries
The most common surgery for bladder control and stress incontinence is the bladder sling. With this procedure, a synthetic material is used to put a sling around your urethra and the muscle connecting it to the bladder. The sling helps to keep the urethra closed when it’s supposed to be closed, such as when you cough. The surgery is highly effective.
Prolapse surgery—such as anterior-posterior repairs, uterine suspension, and vaginal vault suspension—are not anti-incontinence surgeries. However, they can be helpful to women with mixed incontinence and pelvic prolapse, helping them to empty the bladder better and improve overflow incontinence. These procedures are frequently done at the same time as a sling procedure, lifting organs back into place orputting the bladder back to its original shape so it can function normally.
Botox injections have helped treat overactive bladders, but it is usually only offered after other medications and behavioral therapy have been tried and failed. The drug—onabotulinumtoxinA—is the same drug used for wrinkles, but with the bladder injections, Botox can increase the bladder capacity, decrease pressure on the bladder, and halt leakage.
A study in the New England Journal of Medicine stated, “Oral anticholinergic therapy (see medications, above) and onabotulinumtoxinA by injection were associated with similar reductions in the frequency of daily episodes of urgency urinary incontinence. The group receiving onabotulinumtoxinA was less likely to have dry mouth (a common side effect of the medications) and more likely to have complete resolution of urgency urinary incontinence but had higher rates of transient urinary retention and urinary-tract infections.”
Bladder Control: The Bottom Line
There’s no reason to suffer through incontinence issues with adult diapers or panty shields. A consultation with a urogynecologist (or urologist, if you are a man) will help you learn the cause of your incontinence and the myriad treatments available for it.
Starting with behavior modification right through to surgery, you can end the potential embarrassment of a visible urine leak. But be wise. “Always start with your provider, so you can find the cause of your incontinence and learn to use behavior modification to control it. If additional therapies are needed, you will be ahead of the game by leading a healthier lifestyle,” says Dr. Badalian.
NON-INVASIVE THERAPIES FOR URINARY INCONTINENCE
A pessary insertion can be a cost-effective way to control urinary incontinence, if the primary cause is believed to be pelvic-organ prolapse. A pessary is a rubber ring that is inserted into the vagina. It helps hold the organs in place, including your bladder, which helps to prevent urine leakage. Pessaries must be fitted to you by your gynecologist and must be cleaned frequently. In today’s age, many women are choosing less troublesome options.
Posterior Tibial Nerve Stimulation (PTNS) is used to treat overactive bladder and associated symptoms of urinary urge incontinence. PTNS is a minimally invasive procedure that electrically stimulates the nerves controlling bladder function. A needle electrode is inserted into the ankle area once a week for 12 weeks (yes, we said ankle area).
A multitude of studies have shown that this therapy is highly effective for overactive bladder. “The long-term use of percutaneous tibial nerve stimulation (PTNS) is a safe and effective treatment for certain patients who do not adequately respond to anticholinergic medications and behavioral therapy,” says Obgyn.net.
 MGH Study: Hot Yoga May Help Ease Depression Symptoms, but Be Mindful of Health Concerns
MGH Study: Hot Yoga May Help Ease Depression Symptoms, but Be Mindful of Health Concerns  Ramsay Hunt Syndrome
Ramsay Hunt Syndrome 
Loss of bladder control isn't a disease; lifestyle changes may help reduce urinary incontinence.
© Tibanna79 | Dreamstime.com