Sciatica Pain Management: Find the Root Cause and Weigh Your Treatment Options
Shooting pain down the leg from sciatica can be treated, usually without surgery. Here's how to pursue pain management that may make a difference.
“My sciatica is acting up.” This commonly uttered statement refers to pain that starts in the lower back and radiates down the leg. It’s mostly annoying, but it can be debilitating, making effective sciatica pain management an important pursuit.
Sciatica isn’t so much a diagnosis as it is a group of symptoms. It occurs when the sciatic nerve—the largest and longest nerve in the body—is compressed or irritated near where it originates in the spine.
Sciatic Pain: Management Is Key
The sciatic nerve starts as a collection of nerve fibers at the lower portions of the spine—the bottom segments of the lumbar spine (L4 and L5) and the top segment of the sacral spine (S1 to S3). The nerves exit the spinal canal and come together to form the large sciatic nerve, which then runs below a muscle in the buttocks (the piriformis muscle) and down the back of the thigh. Above the knee, the nerve separates into two nerves, which extend down to the foot.
Symptoms of sciatica usually appear in just one leg, but sometimes both. Pain is typically sharp rather than throbbing, and sometimes accompanied by numbness, tingling, and weakness.
What Causes Sciatica Pain?
Management of sciatica pain begins with an understanding of several spine conditions that can cause sciatica. Which one may be affecting you?
- Most commonly, a herniated disk is to blame. The cushioning disks between bones (vertebrae) in the spine have two components: a gel-filled center and a tougher outer portion. Over time, the outer part can weaken, and the gel-filled portion finds a way out, ultimately pressing on other nerves located nearby. The result: a narrowed opening where the nerves live—a problem that produces pain and inflammation.
- Bone spurs can also cause sciatica. As we age, bony projections can develop on the edges of vertebrae. Sometimes they press on a nerve.
- Spinal stenosis—the narrowing of the spinal canal, often caused by arthritis and possibly bone spurs—can also put pressure on nerves, leading to sciatica.
- A condition called spondylolisthesis is another possible culprit. Spondylolisthesis is a defect in which one vertebra slides forward over the vertebra below. This misalignment can cause pain as well as sciatica, usually in both legs.
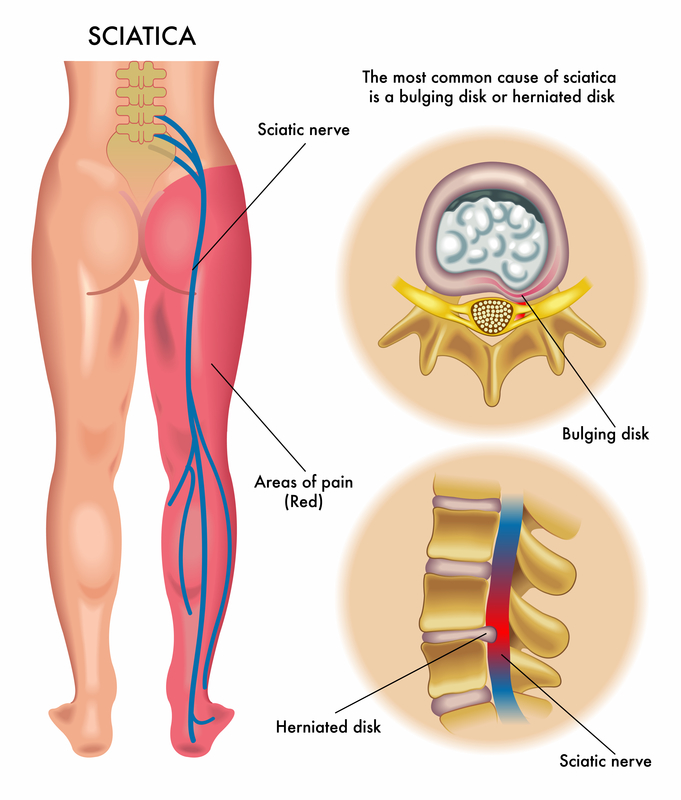
Pictured: a graphic that shows the path of the sciatic nerve. When inflammation develops, pain management is in order. [Illustration: © Rob3000 | Dreamstime.com]
Pinpointing the Cause of Sciatica
If you have what you think is sciatica, see a doctor to get a proper diagnosis. Pain, numbness, and tingling in the lower back and leg may have causes other than those described above. It’s important to find out the real cause.
To sort out the underlying problem, your physician will ask questions about your symptoms, conduct a physical examination, and obtain X-rays. The specific location and character of symptoms can indicate where in the spine the nerve is pinched. For example, compression of the nerve at L4 usually causes symptoms in the lower and inner leg. A pinched nerve at L5 can cause problems that extend to the outer leg and into the big toe.
A magnetic resonance imaging (MRI) test may be done, but generally only if pain persists for six to eight weeks after starting treatment or there is weakness or a change in reflexes that indicate a more serious issue.
Sciatica Pain Management: Treatment Options
Regardless of the underlying cause, sciatica treatment usually starts with conservative measures, such as medications and physical therapy. Medications include nonsteroidal anti-inflammatory drugs (NSAIDs), either over-the-counter (ibuprofen [Advil, Motrin], naproxen [Aleve]) or prescription strength.
Your doctor also may prescribe muscle relaxants (cyclobenzaprine [Flexeril], methocarbamol [Robaxin], metaxalone [Skelaxin]) or medications that address nerve pain, such as gabapentin (Neurontin), pregabalin (Lyrica) or duloxetine (Cymbalta).
Occasionally, short courses (seven to 10 days) of oral corticosteroids are used for their anti-inflammatory benefits.
Physical therapy is aimed at improving flexibility and strengthening the muscles that support the lower back. The aim: to strengthen core muscles.
If pain persists, epidural injections of corticosteroids (powerful anti-inflammatory medications) may be tried. The epidural space, where the injections are directed, is the outermost part of the spinal canal. Specially trained physicians perform this procedure using x‑ray guidance to ensure safety and accuracy. The medication is injected around the inflamed nerve (not into it).
These injections, if effective, may reduce pain enough to help patients progress more quickly to physical therapy, which is the most crucial aspect of the treatment program.
Sciatica Surgical Options
Most people with sciatica recover without ever needing surgery. But if nonsurgical measures prove inadequate, surgery may make sense.
The specific surgery will depend on the cause of the nerve compression. For a herniated disk, a surgeon may perform a microdiscectomy, in which the piece of the disk coming in contact with the nerve is shaved off. The surgery is performed through a small incision in the back.
A laminectomy is a common surgery for addressing spinal stenosis. With this procedure, bone or ligaments that are pressing on nerves are removed to open up the space in the spinal canal.
Prevention
If you’ve had sciatica in the past, it is extremely important to keep up with the exercise program prescribed by a physical therapist, even when you’re no longer feeling pain, to prevent future attacks.
 Vestibular Migraine Diet
Vestibular Migraine Diet  Bone Spurs on the Spine
Bone Spurs on the Spine  Knee Injections for Osteoarthritis Pain Relief
Knee Injections for Osteoarthritis Pain Relief 
For sufferers of sciatica, pain management can help maintain a quality of life. Medication is commonly prescribed; therapy and/or exercise also options short of surgery.
© Kati Molin | Dreamstime.com