Is Low Testosterone to Blame for Your Energy Crisis?
"Low T"—as people call the problem of low testosterone—can sap your strength and vanquish your verve, but so can other, modifiable conditions. Find out what’s causing your symptoms, and know what to expect before you decide on testosterone replacement therapy.
You’re getting older. You’ve lost muscle tone and some pep in your step, and your sex life isn’t what it used to be. Your thoughts turn to low testosterone, and you think about testosterone replacement therapy as a medical fountain of youth, a way to regain your youthful vigor. Trouble is, low testosterone may not be the only reason you’re not feeling up to par.
So, ask your doctor about checking your testosterone, but understand that testosterone replacement therapy should be considered only if your symptoms are from a true testosterone deficiency and after you’ve addressed other potential causes. And, it’s important to understand the risks, benefits, and limitations of supplemental testosterone.
Do You Have Low Testosterone?
Secreted by the testicles, testosterone is the most dominant male hormone, responsible for typical adult male attributes, muscle and bone mass, and sex drive. Most testosterone circulating in the bloodstream is attached to a protein known as sex hormone-binding globulin, while some is attached to another protein, albumin. And, a small amount floats freely in the bloodstream (free testosterone). Free testosterone is the most bioavailable form, meaning it’s the one most easily used by the body, although albumin-bound testosterone can easily be made bioavailable.
Testosterone is measured using a simple blood test of the total testosterone level, although in some cases a doctor may order more specific testing of free or bioavailable testosterone. But what constitutes a low testosterone level is anything but simple.
Experts have yet to reach a firm consensus definition of low testosterone, and reference ranges for testosterone can vary significantly depending on the laboratory completing the test. In general, though, levels less than 300 nanograms per deciliter (ng/dl) are considered low.
Most men begin to experience declines in testosterone starting in their 40s, and some may experience a more precipitous drop after age 60. (Women also have some testosterone—produced by the ovaries and adrenal glands—but at much lower levels than men.)
Signs of Low Testosterone
Low testosterone, or hypogonadism, may cause a number of symptoms in men:
- Sexual: Declines in sex drive; erectile dysfunction, including fewer spontaneous erections
- Body: Fatigue; loss of muscle and bone mass; increased body fat; swollen or tender breasts; hot flashes
- Brain: Depression; impaired concentration
- Sleep: Insomnia
- Blood tests to measure testosterone. The tests should be done in the morning, when testosterone levels are at their peak. Any low reading should be confirmed by a second test given several days later.
- A bone-density scan
- A prostate-specific antigen (PSA) blood test and a digital rectal exam to check for prostate cancer and/or benign prostatic hyperplasia (enlarged prostate)
- Blood tests to measure your hemoglobin level and calculate your hematocrit (the percentage of red blood cells in your blood)
- Follow-up testing within three to six months of starting treatment to make sure your testosterone level has increased and is adequately maintained, and to reassess symptoms.
- Periodic monitoring of your hematocrit/hemoglobin level and prostate health.
However, many of these problems occur in men who are obese, sedentary, or otherwise in poor condition.
Also, an array of factors has been tied to low testosterone and its symptoms. Long-term use of opioid pain relievers (such as hydrocodone and oxycodone) or corticosteroid drugs (prednisone is an example), as well as alcohol abuse, may contribute to low testosterone. Obesity, type 2 diabetes, and obstructive sleep apnea also are associated with declines in testosterone, as are conditions such as chronic lung, liver, and kidney disease.
Before considering testosterone replacement therapy, you and your doctor should rule out these and other potential causes of low testosterone and your symptoms. Correcting underlying problems might help improve testosterone levels and your quality of life.
If your medical history, symptom review, and physical exam warrant it, your doctor may recommend blood tests of your testosterone.
Testosterone levels are highest in the morning and decline throughout the day, so testing must be done early in the morning. And, since testosterone levels fluctuate from day to day and can be affected by an acute illness, any low reading should be confirmed by at least one follow-up test given several days later. Your physician also should order tests to confirm whether low testosterone originates in the testicles or in the pituitary gland or hypothalamus, which prompt the testicles to generate testosterone. (See sidebar below: “Low Testosterone: The Tests You Need.”)
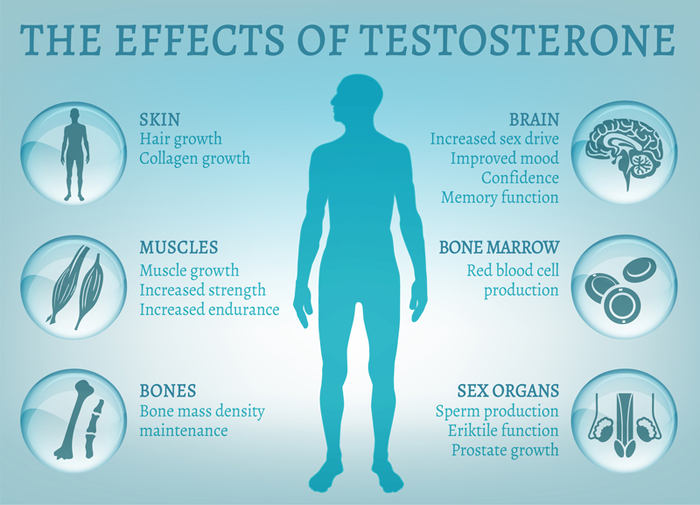
Illustration: © Anna Bocharova | Dreamstime
When Treatment for “Low T” Is Warranted
Over the years, the use of testosterone replacement therapy has soared, thanks in part to direct-to-consumer advertising about the negative effects of “low T” and the benefits of supplemental testosterone. But, testosterone replacement therapy should not be considered (or prescribed) solely as an anti-aging tonic or a hormonal source of rejuvenation.
Although medical societies have yet to reach a consensus on a testosterone level below which testosterone replacement therapy should be started, many experts recommend that treatment be considered solely for men who have levels below 320 ng/dl and have clinical symptoms that can be attributed to hypogonadism. Experts generally advise against using supplemental testosterone in men with only a low testosterone level and no clinical symptoms, as the amount of circulating testosterone that produces symptoms can vary from person to person.
Testosterone replacement is usually administered as a gel (applied daily) or by injection, given every two weeks. Before starting testosterone replacement therapy, undergo a bone density scan, screening for prostate cancer and obstructive sleep apnea, and measurement of your hemoglobin level and hematocrit (the percentage of red blood cells in your blood), in addition to blood tests of your testosterone level.
Testosterone replacement therapy may not be appropriate if you have a history of recurrent blood clots, a hematocrit above 54, a significantly enlarged prostate, uncontrolled sleep apnea, or poorly controlled heart failure. The treatment is contraindicated in men with high-risk or metastatic prostate cancer or breast cancer.
After you begin testosterone replacement therapy, undergo follow-up testing within three to six months to make sure your testosterone levels are adequately maintained and to reassess your symptoms. You also should undergo periodic monitoring of your hematocrit/hemoglobin level and prostate health.
Understand the Limitations and Risks
While research has found that testosterone replacement therapy can benefit men suffering from low testosterone with an identifiable cause, questions remained about whether the treatment helps older men with low testosterone due to no reason other than aging.
So, the National Institutes of Health funded the Testosterone Trials (TTrials), a series of studies to determine the effects of testosterone replacement therapy on several aspects of male aging.
The Ttrials included nearly 800 men over age 65 with two testosterone measurements below 275 ng/dl who were treated for one year with a testosterone gel to raise their testosterone level to the mid-normal range of men ages 19 to 40.
Results from several of the studies—published Feb. 21, 2017, in JAMA and JAMA Internal Medicine—showed that, compared with placebo, supplemental testosterone did not improve memory or other aspects of cognitive function among nearly 500 men with age-related cognitive impairment, but it did increase hemoglobin levels and correct anemia from both known and unknown causes in 126 anemic men. Also, the treatment, compared with placebo, was associated with greater increases in bone density and strength, more so in the spine than the hip.
In earlier findings from the TTrials, supplemental testosterone resulted in increased sex drive and sexual function, and offered some benefit in terms of mood and depressive symptoms, but it had no effect on overall vitality and physical function (New England Journal of Medicine, Feb. 18, 2016).
In 2015, the U.S. Food and Drug Administration recommended label changes to testosterone products to indicate potential cardiovascular risks, based in part on two analyses that found a greater risk of cardiac events associated with testosterone replacement therapy. However, many medical experts cited limitations and flaws in those studies, while also pointing to evidence that the therapy may have a positive effect on cardiovascular health.
In the TTrials, among 138 men, use of supplemental testosterone was associated with an increase in the volume of noncalcified plaque in the coronary arteries (an early indicator of increased cardiovascular risk), but no major cardiovascular events occurred in either the treatment or placebo groups, the study found. And, in a separate study published concurrently with the TTrials in JAMA Internal Medicine, researchers compared the cardiovascular effects of testosterone among 8,808 men with a history of supplemental testosterone use and 35,527 men never treated with testosterone. They found that testosterone replacement therapy was associated with a lower risk of cardiovascular outcomes over an average follow-up period of nearly 3½ years.
The bottom line: Supplemental testosterone is not the elixir of youth, but it can be beneficial when used properly in appropriate patients. Talk to your doctor about any symptoms you’re experiencing, what might be causing them, and whether you should be tested for low testosterone. Then, weigh the pros and cons of testosterone replacement therapy, and decide whether you require treatment.
LOW TESTOSTERONE: THE TESTS YOU NEED
Before starting testosterone replacement therapy, undergo:
During testosterone replacement therapy, undergo:
 Look Beyond the Scale
Look Beyond the Scale  Can Allergies Make You Tired?
Can Allergies Make You Tired?  Does Cooking in Cast Iron Help Iron Deficiency?
Does Cooking in Cast Iron Help Iron Deficiency? 
Low testosterone can lead to increased body fat and affect your energy level, mood, sleep, muscle and bone mass, among other factors.
© Orlando Florin Rosu | Dreamstime